From observations to advice: putting research into practice and bringing practice into research – at global scale
Presented at the 2024 Down Syndrome Research Forum.
A fundamental challenge for individuals and organizations hoping to contribute to meaningful and lasting improvements in the lives of young people with Down syndrome is how to provide families and professionals with timely, relevant, and actionable advice, informed by the latest available evidence.
Very little advice can be both simply stated and broadly applicable. Much depends on current levels of development across multiple domains – a challenge compounded by wide variability in rates of progress among children with Down syndrome. Traditionally, advice providers have documented interventions in written guides and handbooks, perhaps accompanied with videos and presentations.
In general, this approach leaves it to families and educators to work out how to apply advice appropriately for each child. Our experience indicates that this is often insufficient to ensure consistent and successful implementation in practice.
Meanwhile, there is a lack of current data to better inform guidance, or to evaluate and evolve interventions over time, or to explore the consequences of social, economic, cultural or policy differences across populations. Much of the available data involves small samples with narrow recruitment criteria and is increasingly dated.
In this presentation, we report on systems that we have developed to collect observations, to generate personalized advice and guidance, and to build datasets on many aspects of development. We will describe how these systems can collect observations from many sources, including family/educator input via web sites or apps, or more automated data collection within apps. We will also describe how we are developing models of speech and language to generate highly specific guidance about appropriate target vocabulary and grammar, speech sounds and speech patterns, helped by recent advances in computational linguistics and machine learning. We will discuss how predetermined advice algorithms might be augmented with reinforcement learning approaches to be more responsive and self-optimizing, and how these approaches might be evaluated and monitored. We will outline our plans and explore how families, organizations, professionals, and researchers can collaborate to help evolve, extend, and utilize these systems to deliver more individualized and better targeted support for young people with Down syndrome everywhere.
A central goal of research into Down syndrome is to improve outcomes.
For research to change outcomes, it must influence the actions of those who support young people with Down syndrome at home, in school and in their communities.
Research has transformed outcomes
Over the past 50 years, clinical, developmental, and educational research has helped to transform outcomes for many people with Down syndrome.
In some countries, clinical research has helped to lift life expectancy from 30 to 60 years, while developmental and educational research has helped some children achieve levels of language, literacy and numeracy considered unachievable 50 years ago.
Down syndrome research over the next 50 years will be different from past research. It will explore new topics and old topics in new ways – adding to and updating our current understanding. Early intervention and education will also be changing.
How can we maximize the benefits of research over the next 50 years?
Challenges
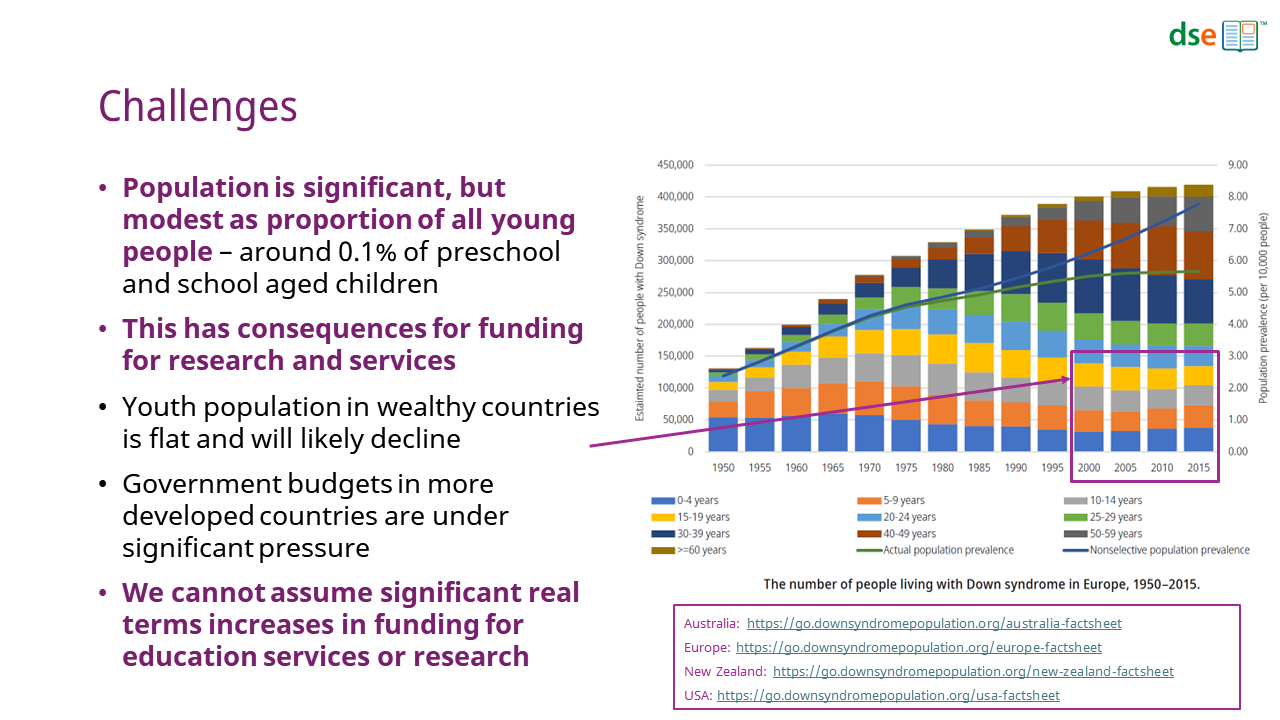
The population of young people with Down syndrome is significant but modest as proportion of all young people – around 0.1% (1 in 1,000) of preschool and school aged children have Down syndrome.[1–3]
Families are unlikely to be familiar with the condition before the arrival of a baby with Down syndrome. On average, a primary school teacher in a mainstream school may teach a child with Down syndrome once in approximately 40 years of teaching.
The population of people under 20 years of age in more wealthy countries has not increased for many years and is likely to decline.[1–3]
Government budgets in more developed countries are under significant pressure, suggesting that we cannot assume any significant real terms increases in funding for education services or research in the foreseeable future.[4]
Largely due to funding constraints, Down syndrome research studies are often small, often involving only a few dozen children in one location.[5,6] There are risks that some studies may have insufficient power to detect differences and that some may be not be representative of all members of the Down syndrome community.
Most studies are only funded for a limited period. As a result, there is very little longitudinal data published.
Most study participants are from Euro-American middle class families living in Western, educated, industrialized, rich and democratic societies that may not be representative of other countries or people from different backgrounds.[7,8]
It takes time to plan, find funding, conduct, and report research. Most projects take more than 3 years, often more. There is then a further delay for findings to be incorporated into routine practice.
Are there ways we could do research more quickly and with larger and more diverse populations, yet within realistic budgets?
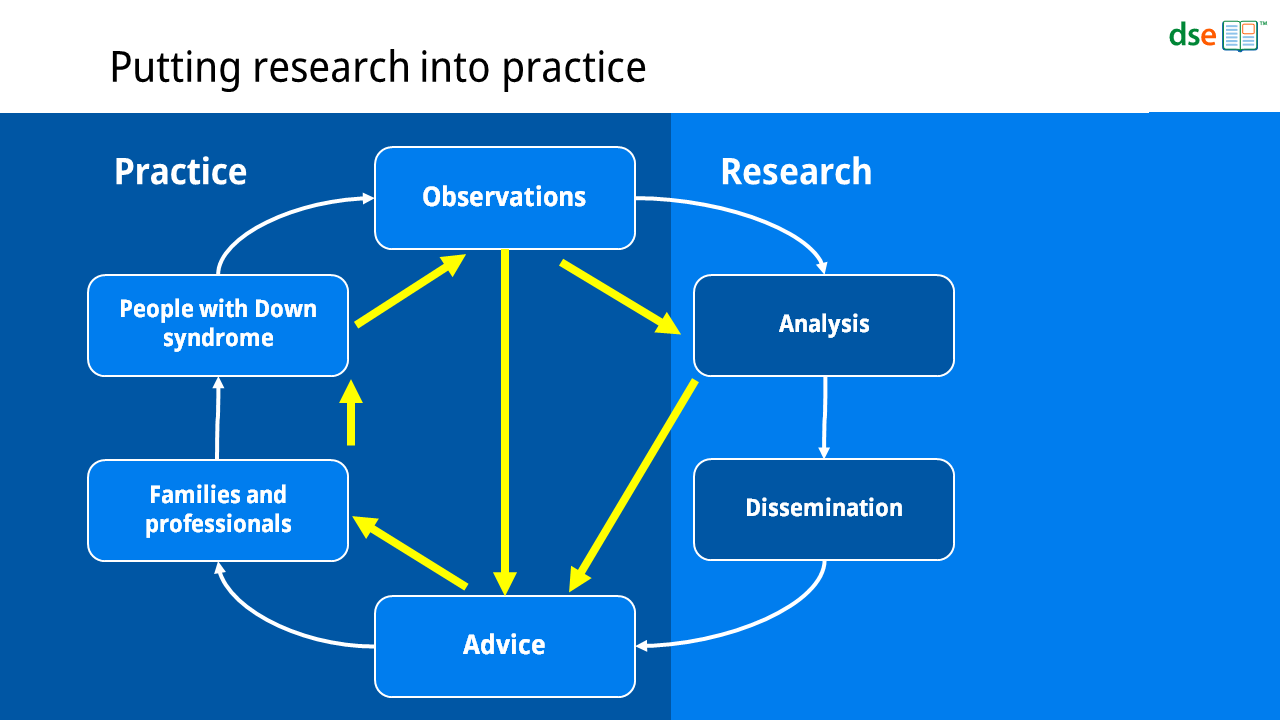
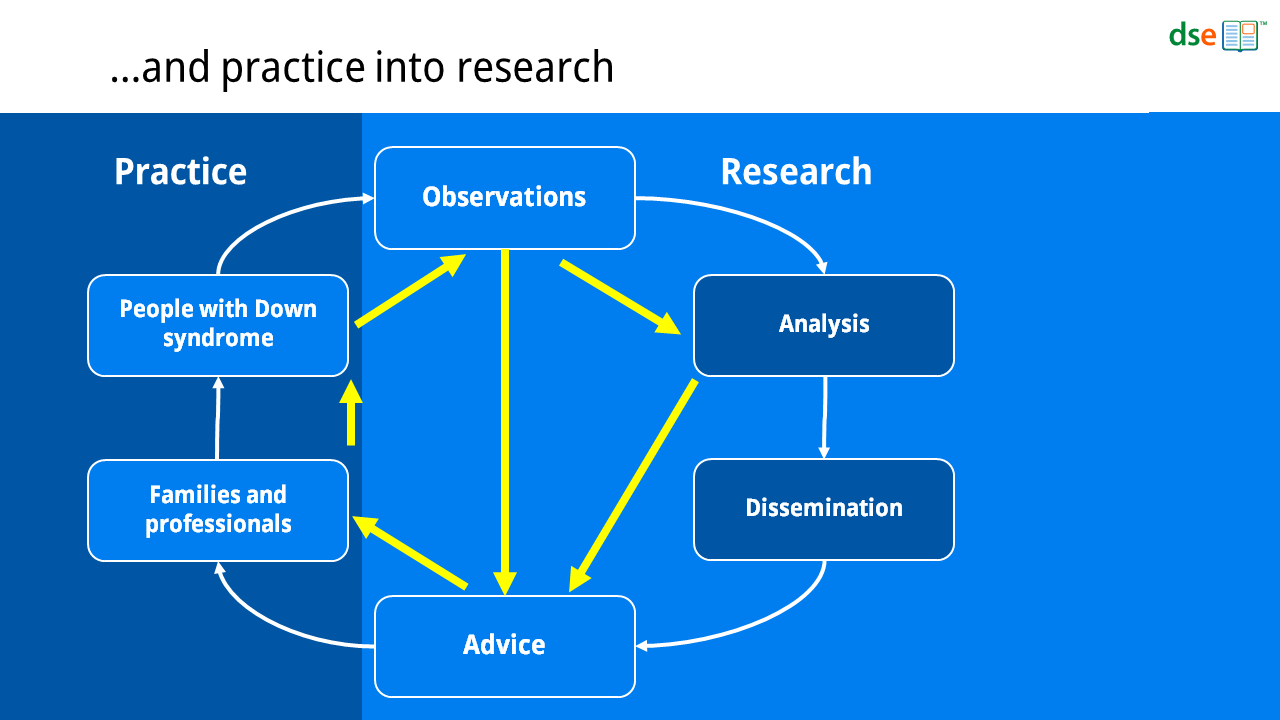
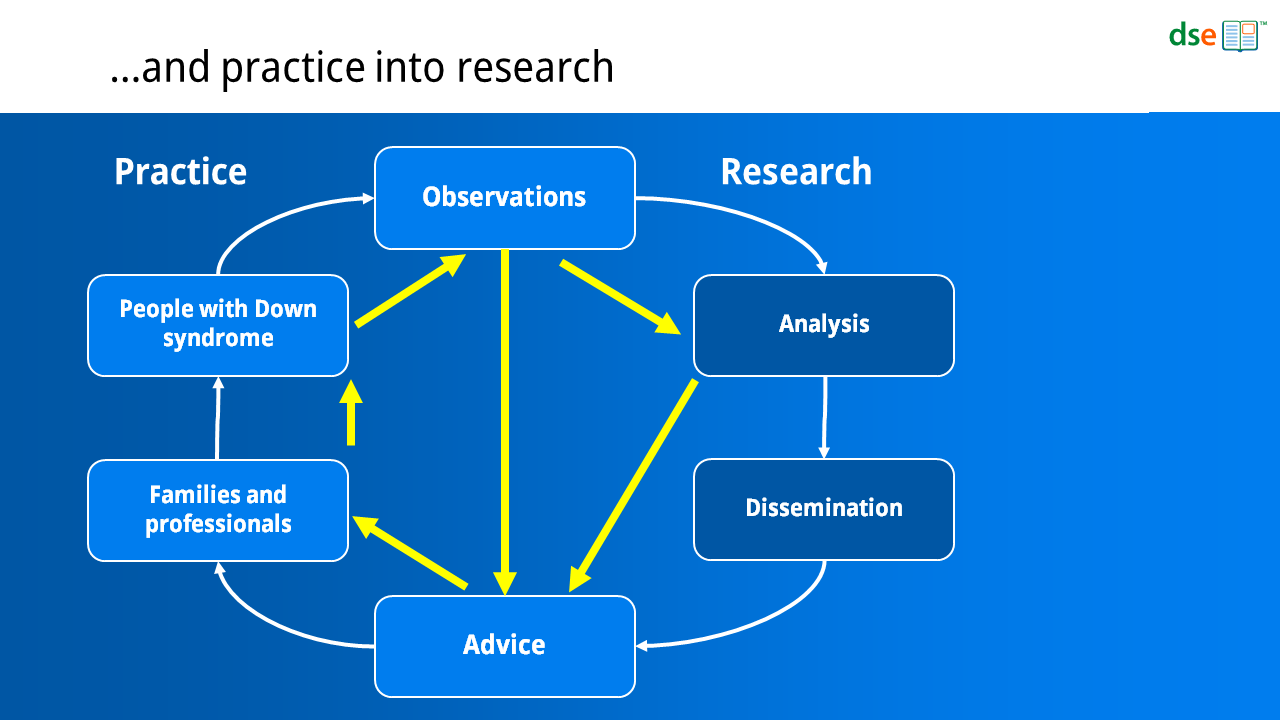
Putting research into practice
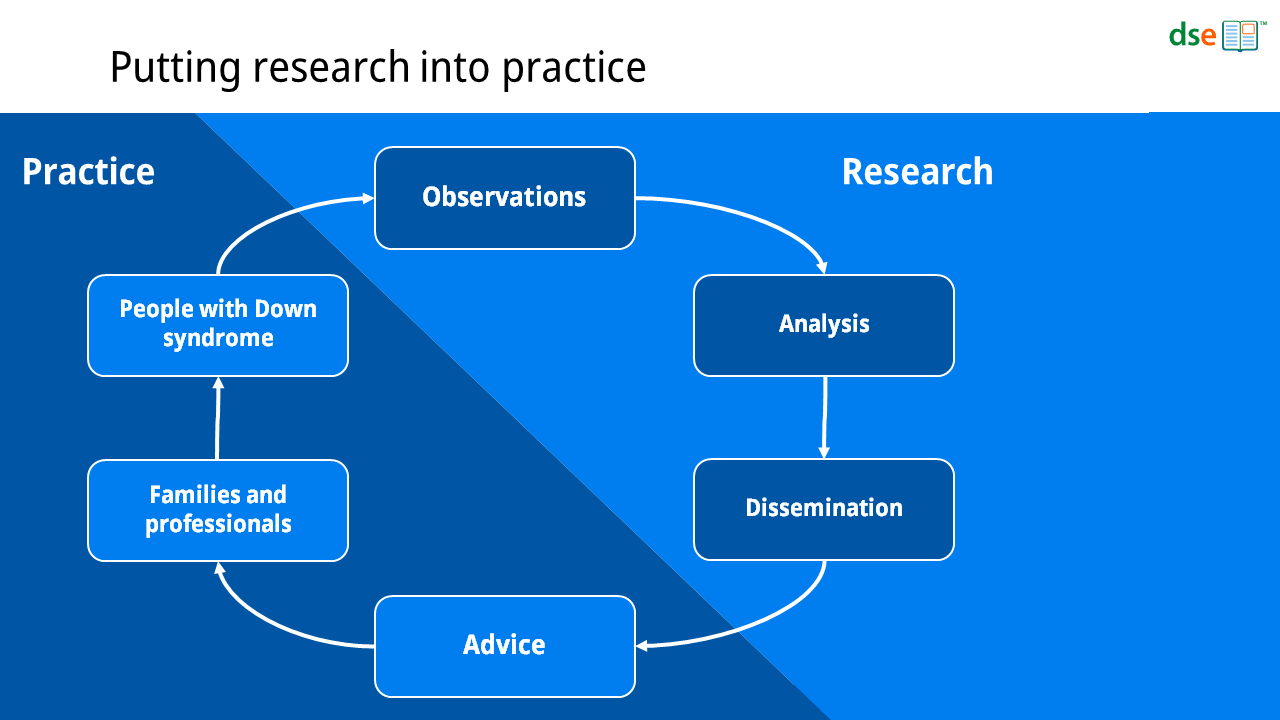
Today, research is generally undertaken through discrete, time-limited projects that end with the dissemination of their results. Researchers seek funding for a defined study, conduct that study and report their findings. They then move on to find funding for their next study.
Some research studies result in reports or guidance aimed at families and professionals – in addition to the scientific papers. In general, however, most research findings influence practice through printed and online publications and training courses that summarize and synthesize what we understand about the condition and the implications of this for effective care and support. These resources guide families and professionals and are usually published by nonprofit organizations.
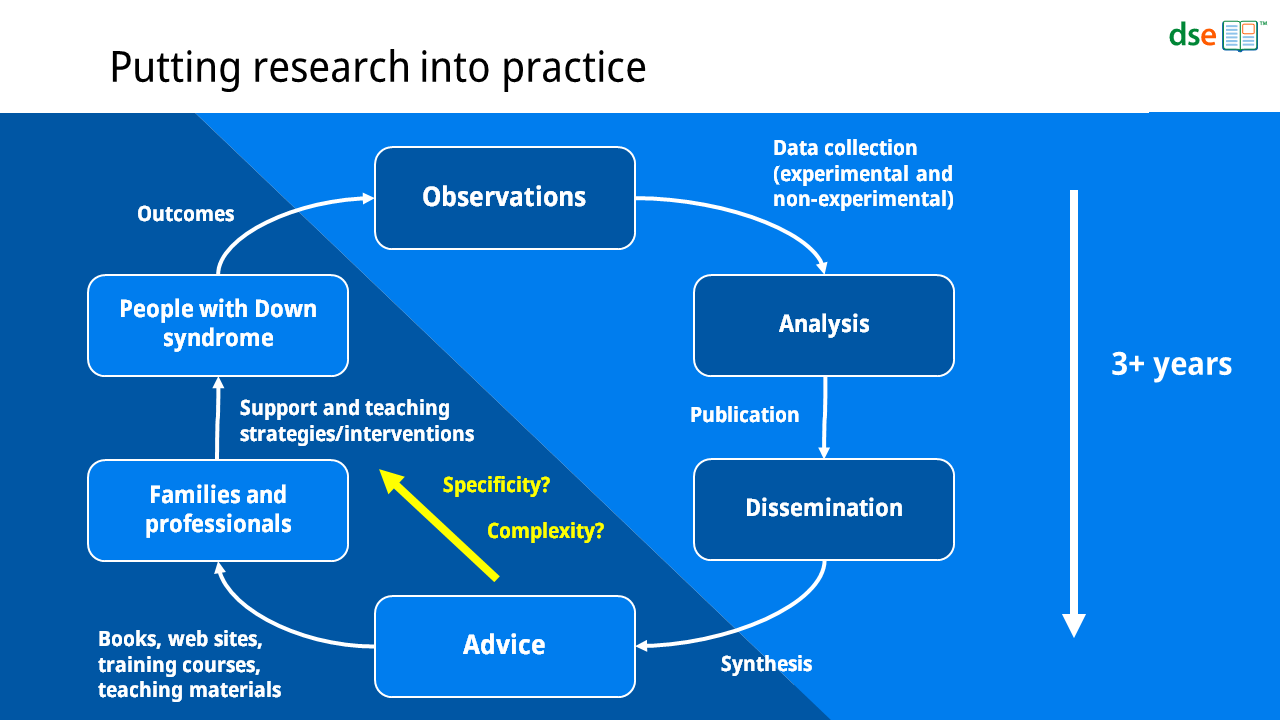
Some advice is generic – that is, it applies to all children with Down syndrome. Some advice is limited to certain groups – for example, children of certain ages or children with certain medical conditions. Much advice has preconditions, such as the child’s current stage of development in a particular domain or on a defined measure.
As our knowledge of Down syndrome grows, we find more and more opportunities to help. However, as the range of the issues we understand grows and as our understanding of these issues deepens, so too does complexity for professionals and families.
Many families already find it difficult to review all of the information and advice that is available to them and are often unsure how to apply it to how they support their child.
For some time now, we have been thinking about ways we might be able to both accelerate scientific progress and simplify how advice is put into practice.
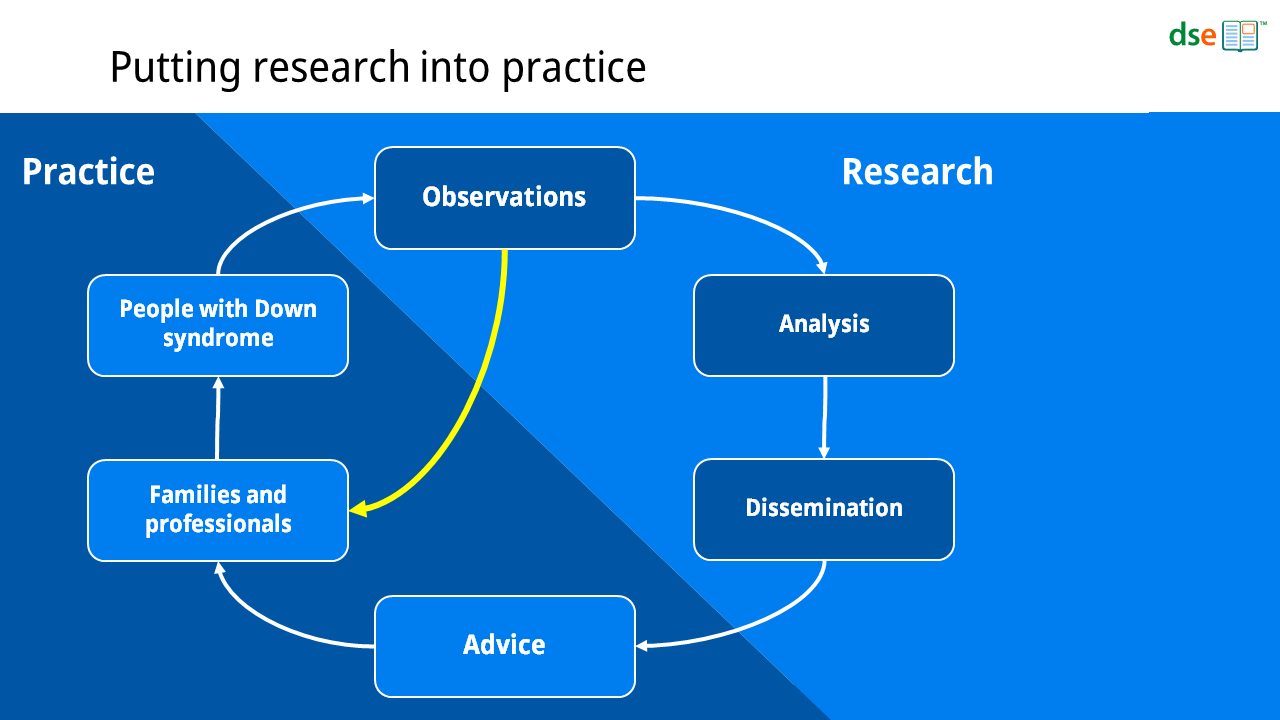
Parents and professionals observe children’s development and monitor progress all the time – sometimes formally with structured record keeping, but most often informally. We all monitor our children’s development against common milestones, we think about their skills in a variety of domains and what this means for the next steps in their learning.
Observing our children and how they are progressing and how we can help to nurture their development is a natural and everyday part of parenting.
So, what would happen if we could collect some of these observations as a routine part of daily life, classroom teaching and therapy provision?
The first thing this could enable would be personalized advice that is appropriate for that child at her/his current stage of development. This reduces the amount of information that a parent or professional must review. In this context, advice can be specific, detailed, and concise.
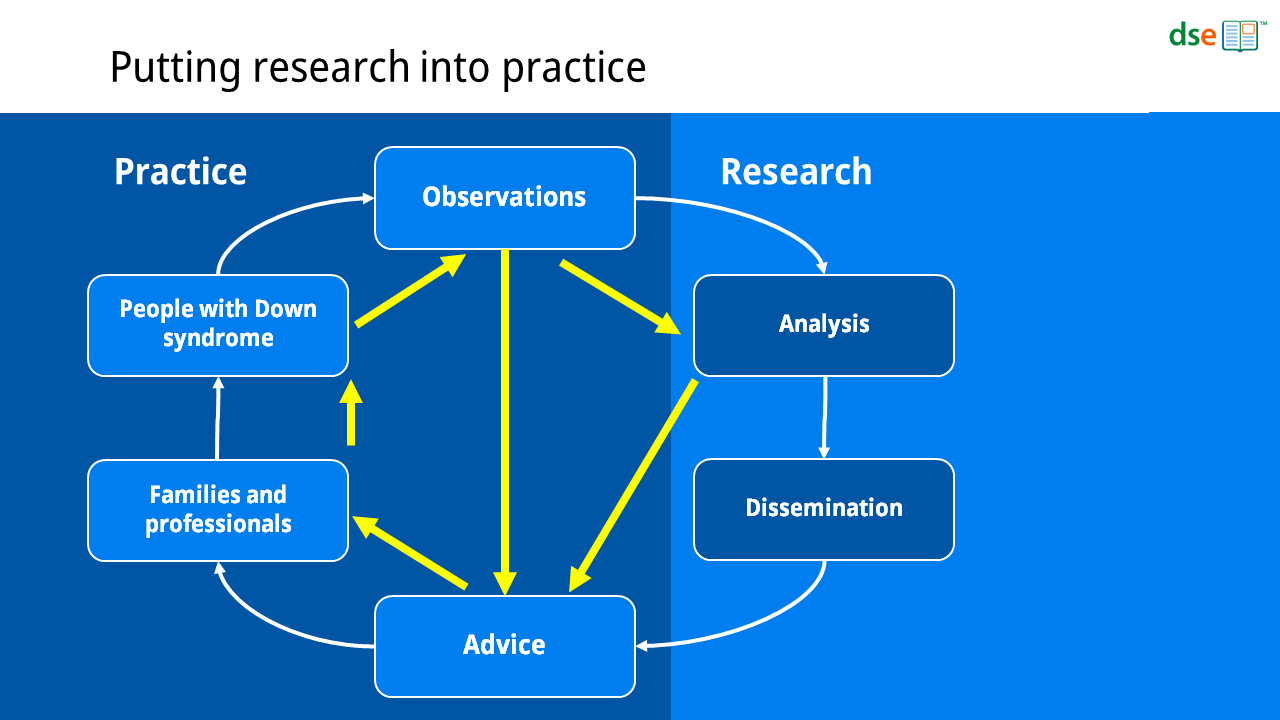
The second thing this could enable would be data collection on a scale unachievable in research projects today. The marginal costs of additional data collection, storage and advice generation are small and can feasibly scale to support many hundreds of thousands of children.
Thirdly, this could speed up the process of bringing evidence into advice.
In doing so, we could both improve and accelerate the research-practice loop.
From observations to advice
For some years now, we have been developing systems to do this.
In the coming months, we will be beginning to release new services built on these systems.
The first services will offer families of preschool children opportunities to track their children’s progress on a number of early development milestones, vocabulary and grammar learning, and speech measures.
As they record their child’s progress, families will be able to access advice about supporting their child’s early communication, speech and language development. This advice will be tailored to their child’s current stage of development, based on the observations recorded.
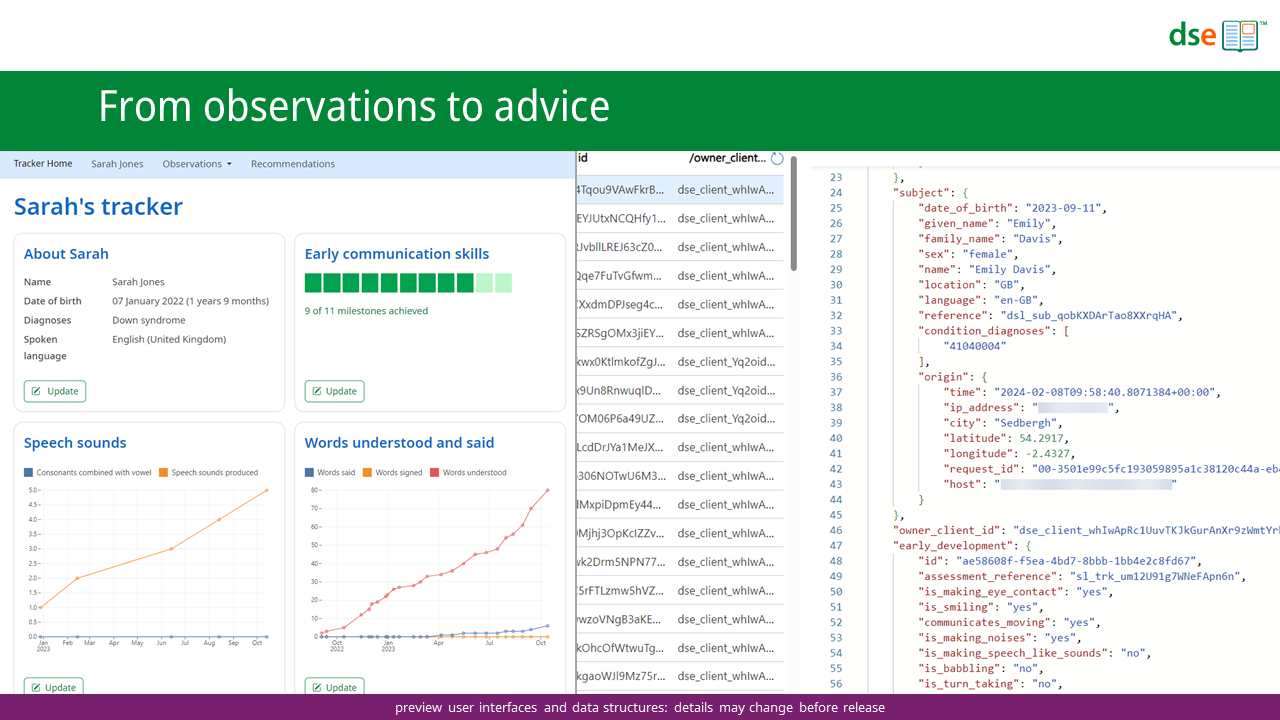
We start with systems for collecting observations.
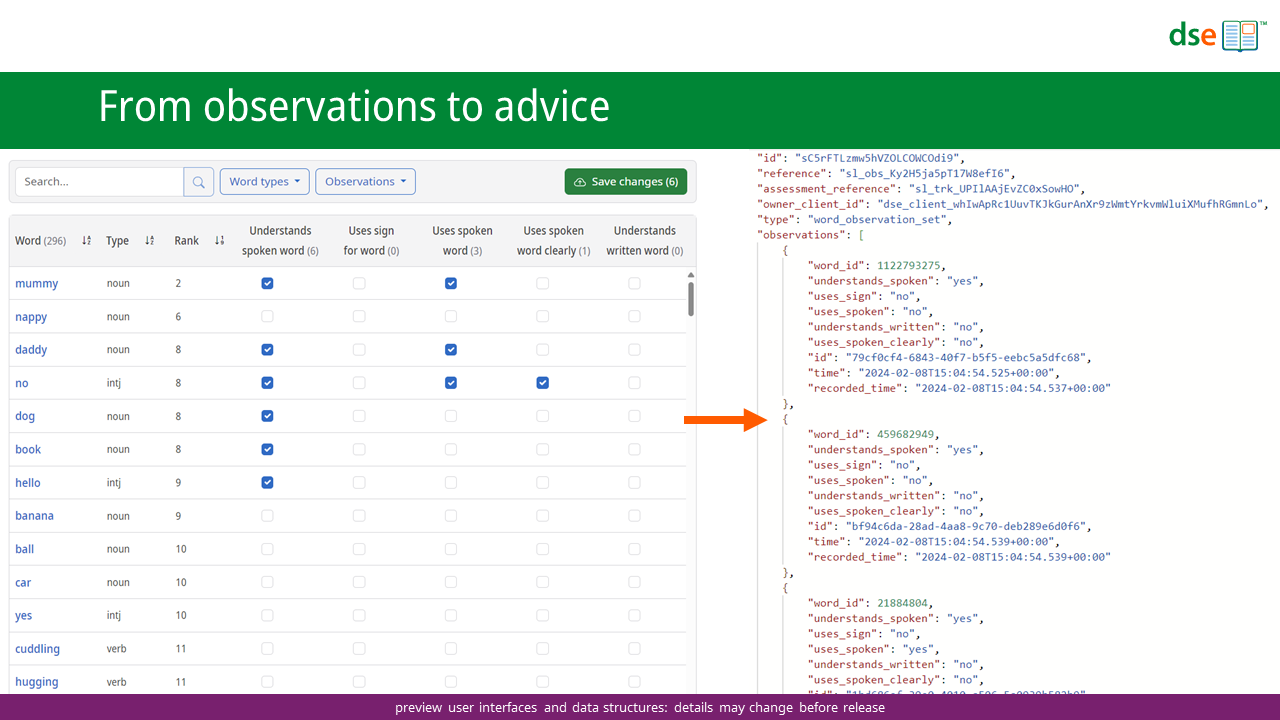
An observation is a value that measures something of interest in relation to the child at a specific point in time. This could be a binary or categorical value, or a count, or a real number. It could also be a more complicated piece of data, such as a voice recording or a video observation.
Observations can be collected in a variety of ways. These include forms on web sites or in apps that parents or professionals can complete.

Observations may also be collected via apps where children are engaged in teaching activities. Here, we can directly record if a child succeeds at a particular task. We can also record the frequency and the duration of teaching activities and collect audio and video samples.
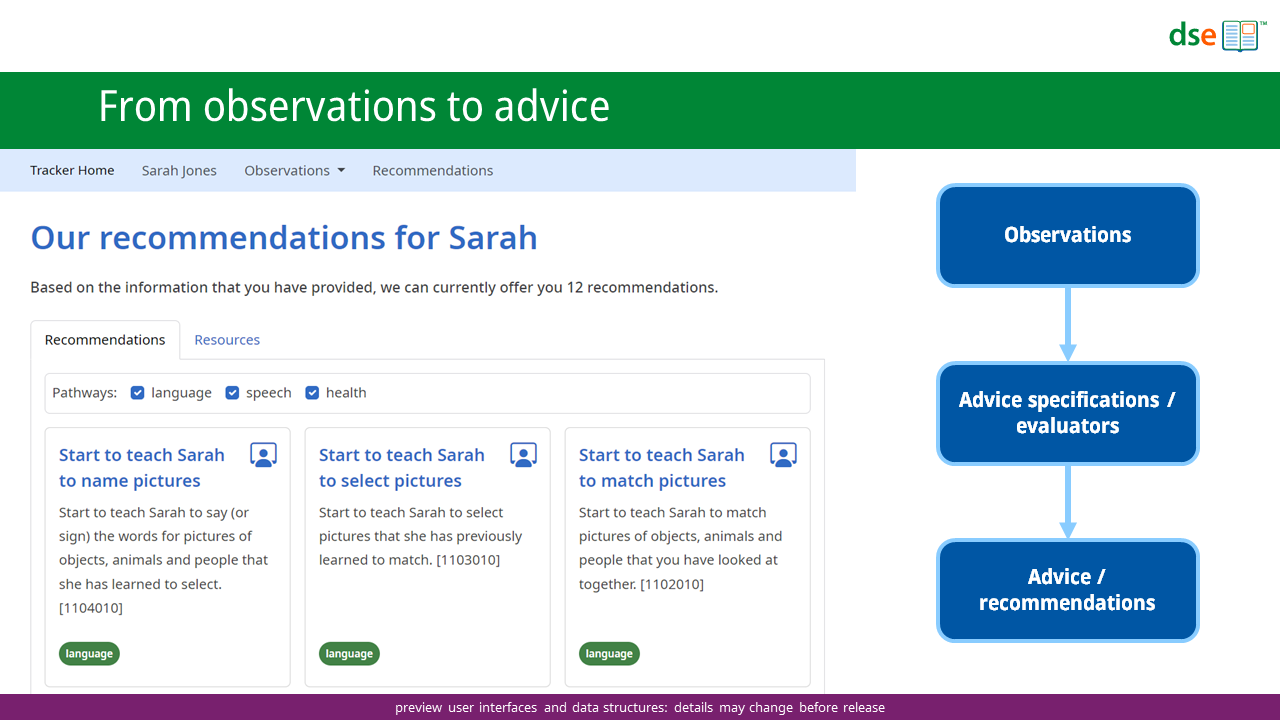
Having collected observations, we can select appropriate advice, given what we have been told about the child.
To do this, we take a snapshot of the observations for a child and pass this data through a series of advice evaluators. These compare pre-defined advice specifications against the observations to decide if a particular piece of advice should be presented.
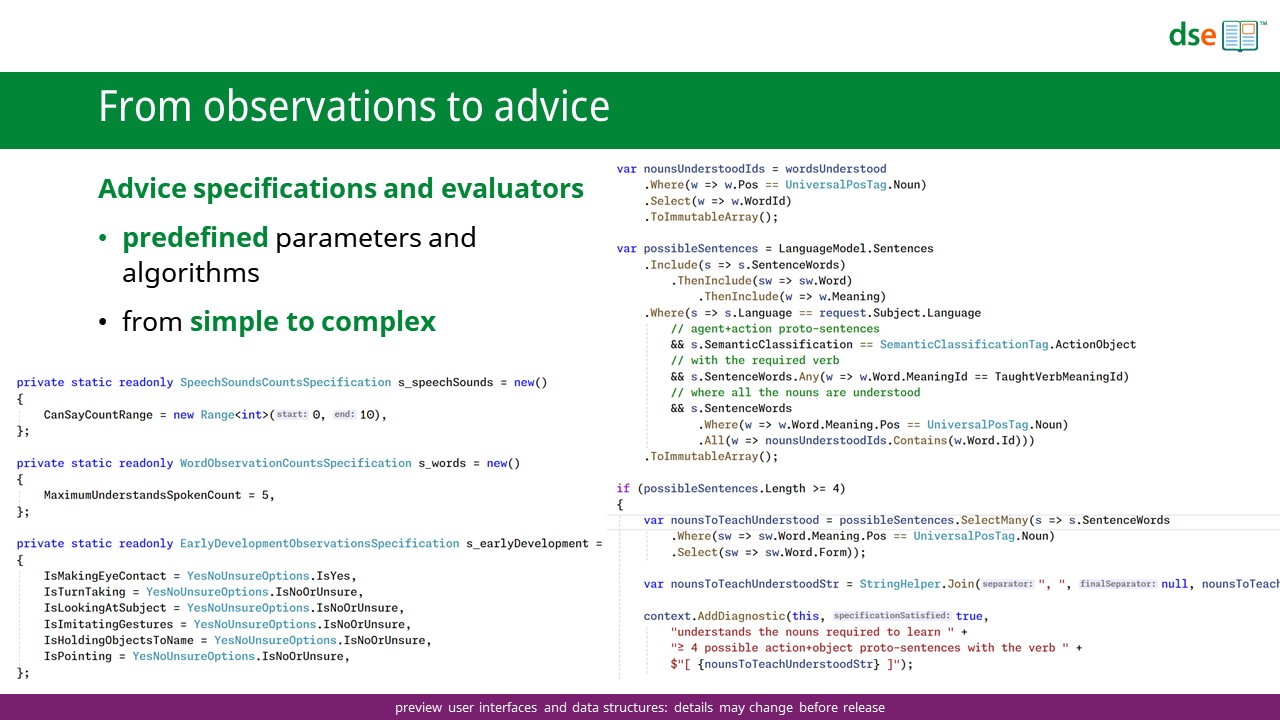
Some specifications can simply depend on a single binary variable – for example, “does the infant make eye contact?” (yes/no).
Most specifications are more complicated and draw on a variety of measures across multiple domains – for example, speech sounds produced in isolation, words understood and number of action + agent phrases understood.
Our initial focus is advice for speech and language development in infancy and early childhood, as these are areas where we already have data and step-by-step advice to build on. However, the systems are designed to accommodate any observation that can be encoded digitally across any developmental domain and age range.
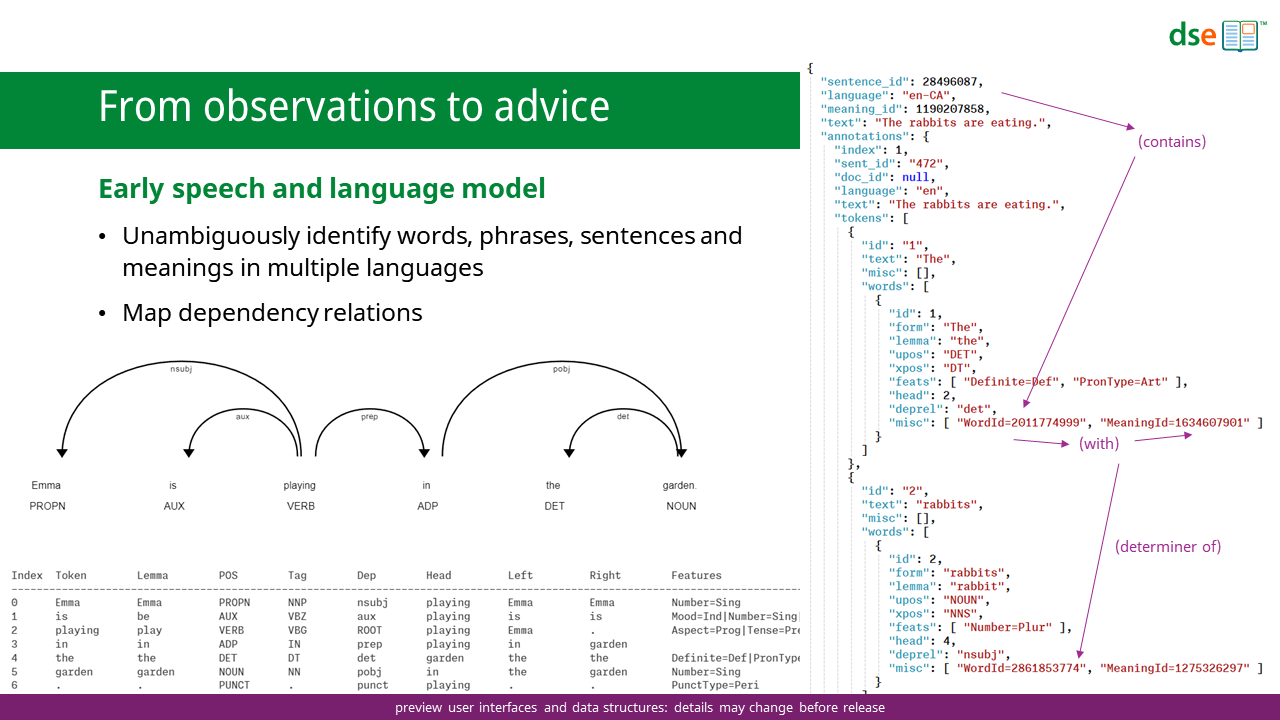
To define language observations and advice specifications, we have begun to build a rich model of early speech and language including single words typically learned early in development, simple phrases and sentences, together with phonetic transcriptions.
The model unambiguously identifies words in different languages and links them to their underlying meanings.
The model maps the words in phrases and sentences in different languages to underlying sentence meanings and structures, including semantic dependencies and features.

This model enables us to execute queries that span speech sounds and words and match results to the observations we have for each child when formulating individual advice.
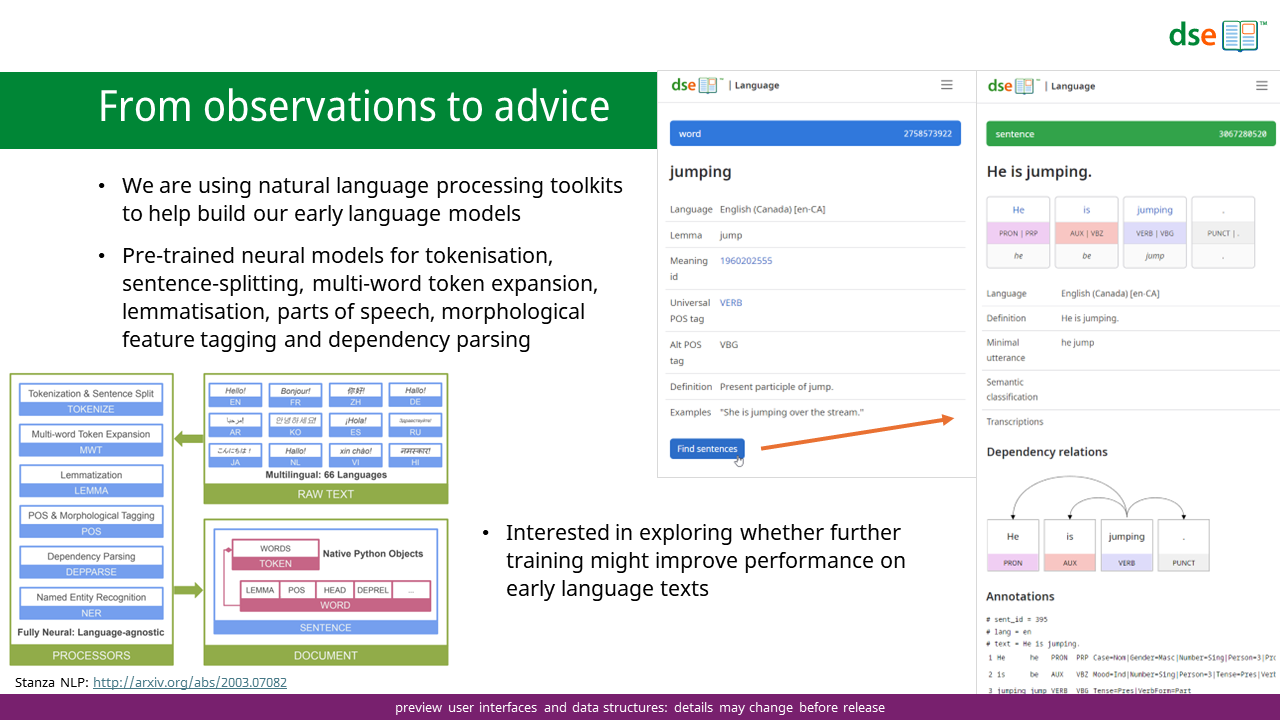
We are using natural language processing toolkits to help build our early language models.
These toolkits offer pre-trained neural models for tokenization, sentence-splitting, multi-word token expansion, lemmatization, parts of speech, morphological feature tagging and dependency parsing.[9,10]
We have found that these toolkits can achieve high levels of accuracy with the simple sentences that are the focus of early language teaching. We are interested whether further training with early language texts might further improve performance.
Our goal is to build a platform that can serve families everywhere. In predominantly English-speaking countries there are around 97,000 children under the age of 15 years living with Down syndrome. Globally, there may be 1.5 million children with Down syndrome in this age range.
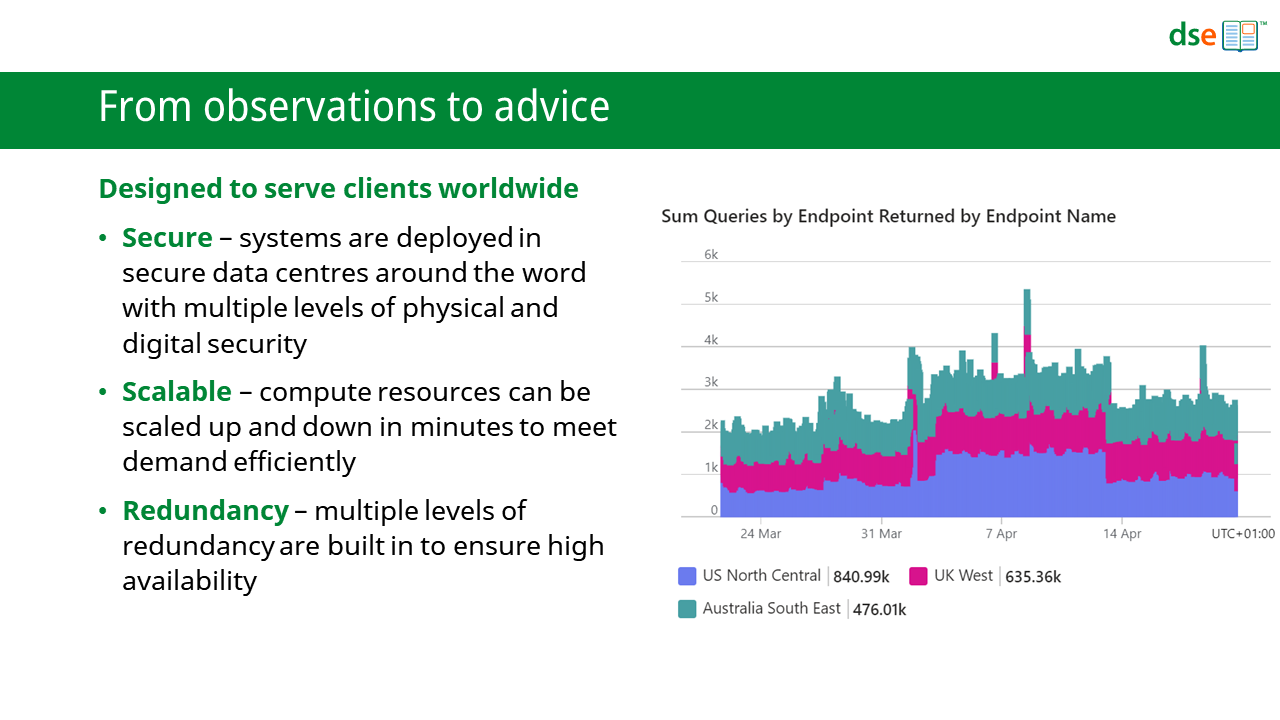
We have therefore designed these systems to potentially scale to tens or even hundreds of thousands of simultaneous users.
We are deploying these systems in regional clusters – initially close to predominantly English-speaking populations. These clusters operate largely independently and reduce request latencies by being closer to users.
They are hosted in secure data centres with multiple levels of physical and digital security meeting international regulatory standards and best practices.
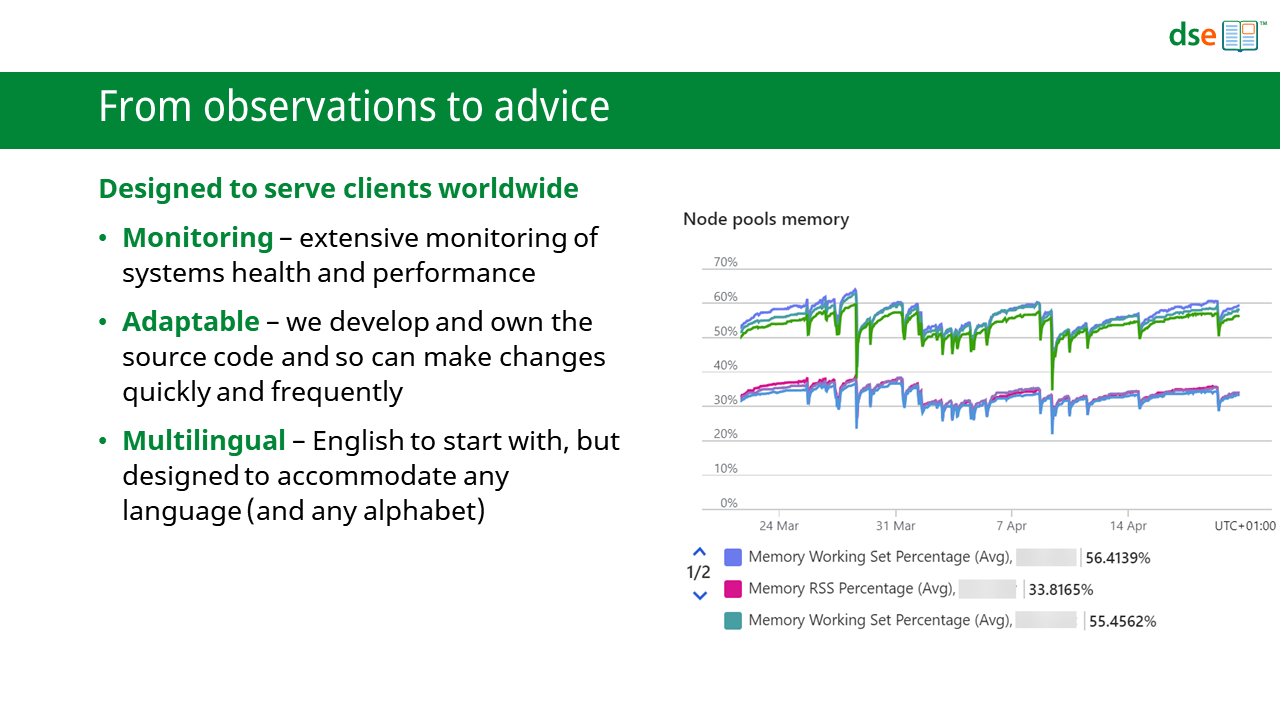
The health and performance of the systems are continually monitored.
If a regional cluster fails, traffic is automatically switched to the next-nearest functioning cluster. Within clusters, services are distributed across multiple compute resources for further redundancy.
We have developed all the key components of these systems, and so we own the source code. We can therefore make changes easily, frequently and quickly.
We are starting with English, but everything has been designed to accommodate any language.
In summary, we have developed systems to collect everyday observations and then use these observations to offer more precise, more relevant, and more timely advice.
This advice is personalized for each child using a data-driven approach with pre-determined algorithms based on the best available evidence.
As new research findings that might impact the advice are reported, the advice specifications can be easily updated. We believe that this will improve the quality of advice we can offer and help to bring research into practice more quickly.
In addition, the data collected by our systems should also inform better advice in the future.
In support of this, we want to make the data collected as openly accessible as possible. We also want to share our infrastructure to support ongoing research and to facilitate the delivery of new interventions.
We hope that openly sharing data will further accelerate and improve the research–practice loop with data sets available for research regularly updated to reflect the latest observations.
These systems will also offer opportunities to conduct larger studies more cost-effectively. We hope to make it as straightforward as possible to create add-ons that can offer customized data collection and feedback to users opting into specific studies, and to connect therapeutic or educational apps or devices to the systems.
We are also developing services for educators and therapists supporting multiple children where they can record their own observations and share them with the children’s families (and where families can also share their observations).
In so doing, we hope to embed continuing research more closely in the daily lives of people with Down syndrome and their families, at home and at school and in therapy sessions.
We hope this may make research an ordinary part of practice in early intervention and education.
Most of all, we hope that we can better help families and professionals improve outcomes for many thousands of children and young people.
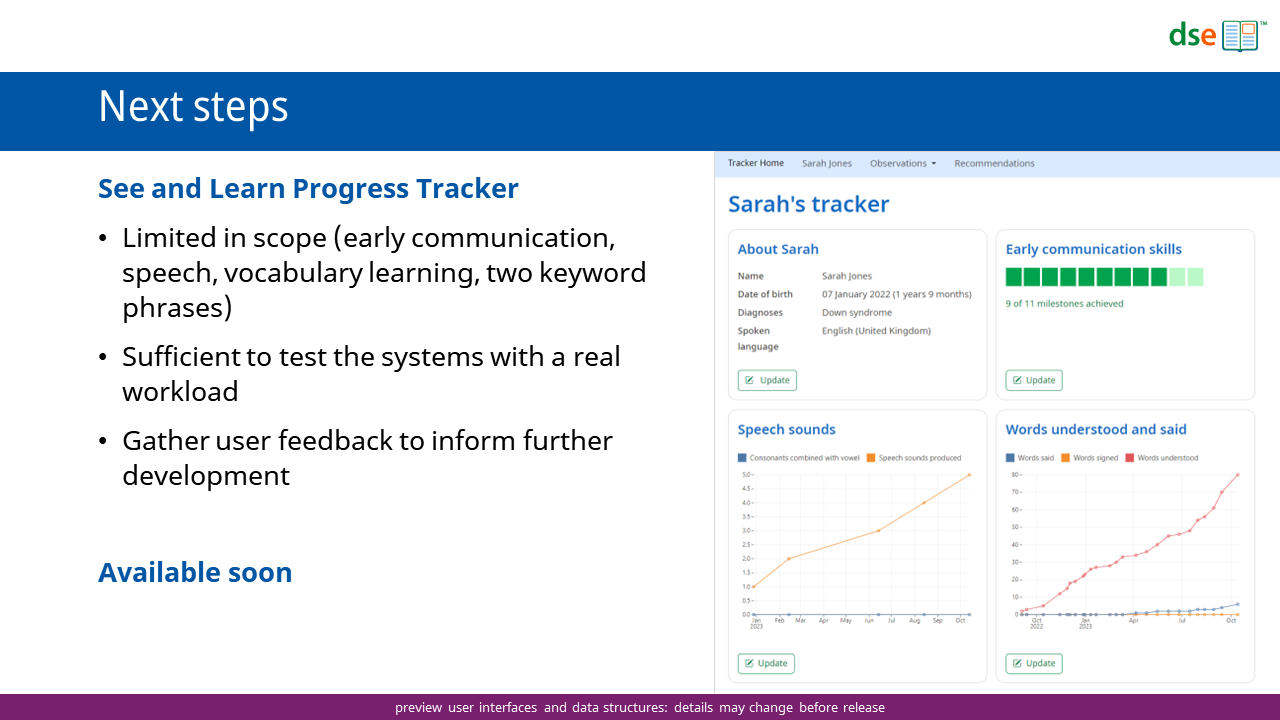
So, what are the next steps?
We will shortly launch the See and Learn Progress Tracker.
This service is built on these new systems but limited in scope. However, it is sufficient to test the systems with a real workload and to provide a valuable service for families.
We hope that it will provide valuable feedback to inform the continuing development of these systems and more fully-featured progress tracking and advice services.
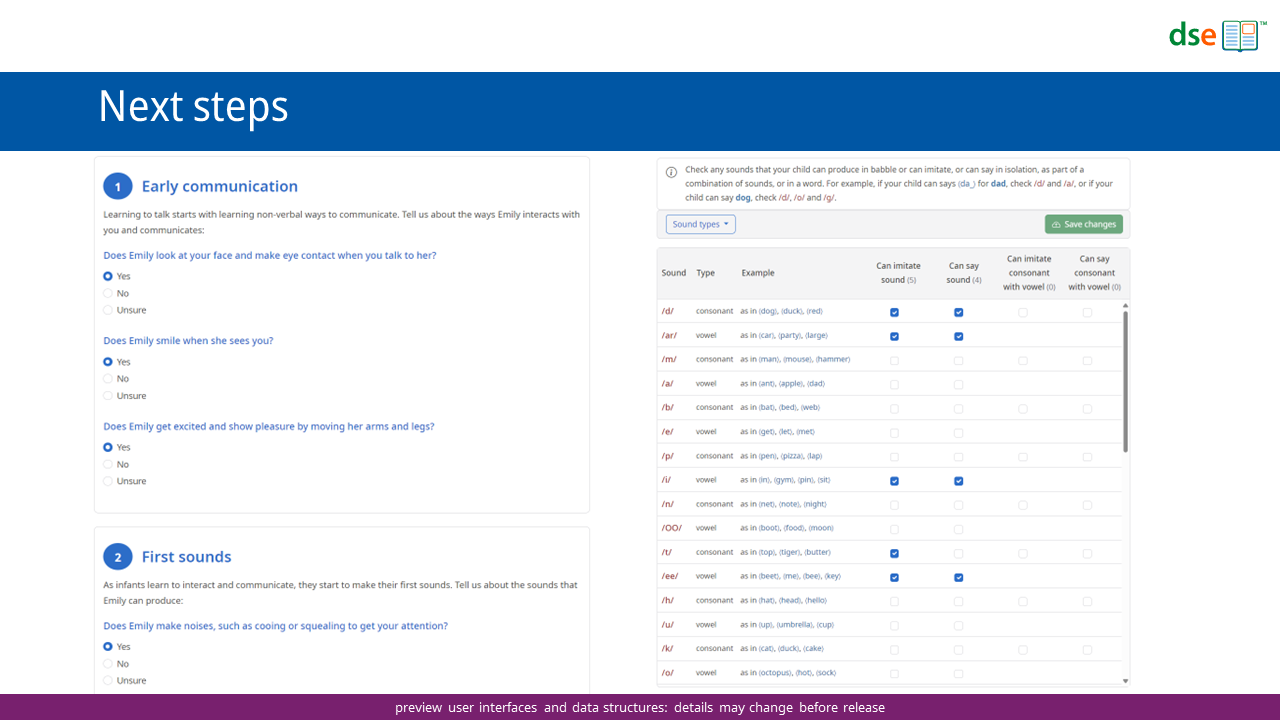
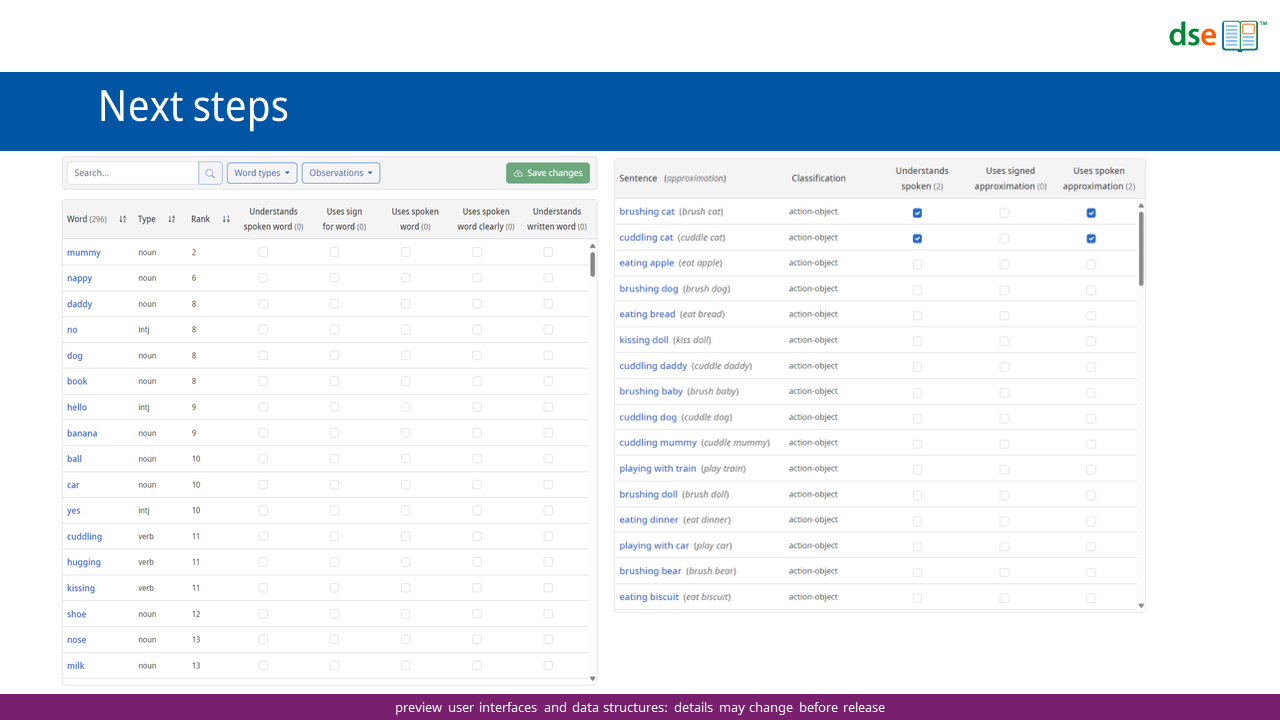
The See and Learn Progress Tracker will collect observations of early communication milestones, speech sound production, vocabulary learning and two keyword comprehension.
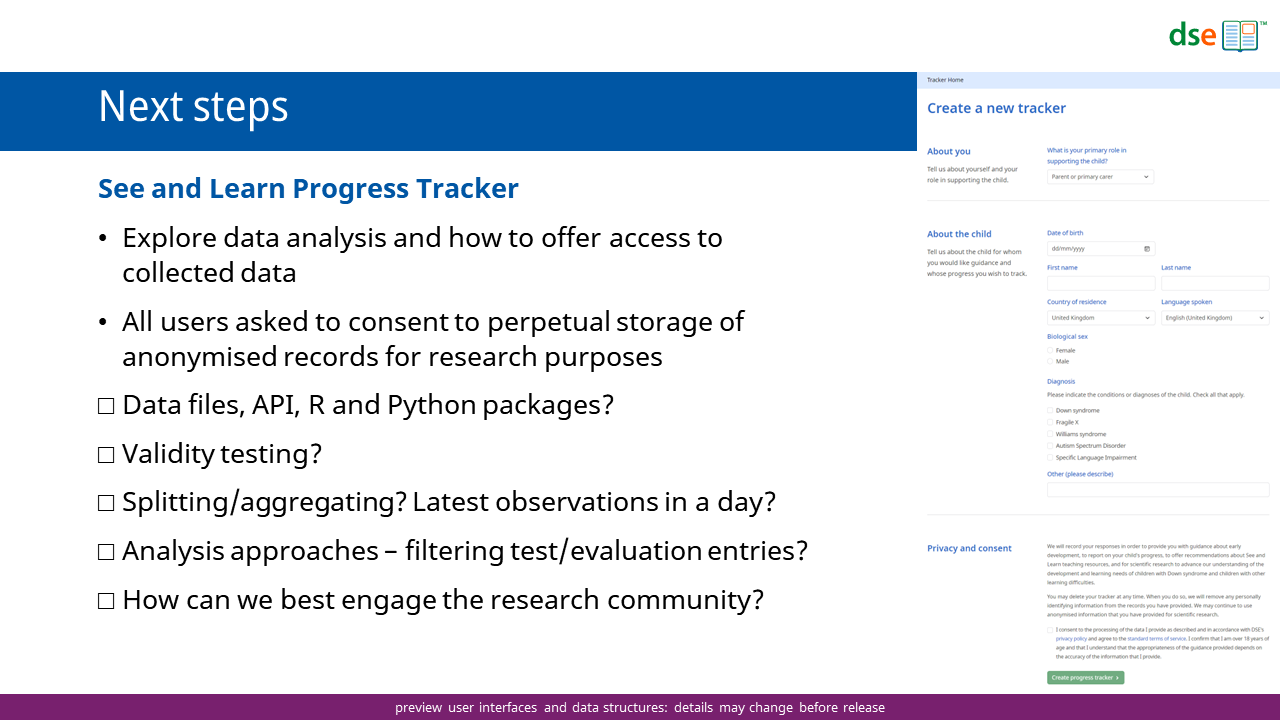
We hope this will also give us real-world data that will allow us to explore data analysis approaches and how best to offer access to the data.
Would unfiltered data files be helpful (they may get very large) or would an interface that can provide filtered data sets be more useful? Would packages to make this easy to access from R or from Python be helpful for researchers?
How should we approach validity testing? Parent-reported measures have been widely used in Down syndrome research for some time.[11–13] How might we assess the validity of parent reports using online tools and apps in many countries?
How should we approach analysis? If advice and progress tracking is openly accessible to parents and professionals, how do we determine when entries are ‘for real’ or for testing or evaluation?
How do we best engage the research community in developing and evaluating best practices?
Next, we plan to launch more fully featured advice and progress tracking services that will also be accessible via mobile apps.
We want it to be as easy as possible for parents and professionals to note down observations, and to be able to reach for personalized advice at any time.
Smartphones are the most widely used internet-connected devices, so we believe that offering convenient and intuitive apps on phones (in addition to other platforms) is important for reaching the maximum number of people.
We are starting to consider how we might make the advice specifications adapt to new data – rather than relying on pre-determined algorithms derived from past data. For example, as word-learning patterns change over time and in different cultures, advice should automatically reflect these changes.
Similarly, we are beginning to investigate if reinforcement learning techniques14,15 could be used to fine-tune advice – perhaps varying the frequency of consolidation activities according to how much rehearsal that child appears to need.
We are also starting to think about how experiments might be conducted using the advice systems by trialling different advice with different groups – and how we can open the platform to researchers for their own experiments.
We are eager to work with colleagues and families around the world as we continue to evolve these systems.
We are particularly interested in engaging with anyone who is interested in:
- how the platform might be extended across more developmental domains and across more age groups
- how we might approach data analysis – potentially with large volumes of data – and how we might automate this and make data openly available
- helping with translations and adaptations
- developing and testing decision-making algorithms – particularly algorithms that will adapt to new data, including self-learning algorithms
- new observation and intervention paradigms – there are many opportunities for new and innovative approaches to intervention – from speech recognition to large (and small[16,17]) language models for individualized conversations and story books
If you would like to follow our work in this area, or (even better) get involved:
- Join our community: https://community.down-syndrome.org/c/progress
- Updates: https://www.down-syndrome.org/progress/
- Email: progress@dseinternational.org
References
- de Graaf, G., Buckley, F. & Skotko, B. G. Estimation of the number of people with Down syndrome in the United States. Genet. Med. Off. J. Am. Coll. Med. Genet. 19, 439–447 (2017).
- de Graaf, G., Buckley, F. & Skotko, B. G. Estimation of the number of people with Down syndrome in Europe. Eur. J. Hum. Genet. EJHG 29, 402–410 (2021).
- de Graaf, G., Skladzien, E., Buckley, F. & Skotko, B. G. Estimation of the number of people with Down syndrome in Australia and New Zealand. Genet. Med. Off. J. Am. Coll. Med. Genet. 24, 2568–2577 (2022).
- Drayton, E., Farquharson, C., Ogden, K., Sibieta, L. & Tahir, I. Annual Report on Education Spending in England: 2023. https://ifs.org.uk/publications/annual-report-education-spending-england-2023 (2023).
- Smith, E., Hokstad, S. & Næss, K.-A. B. Children with Down syndrome can benefit from language interventions; Results from a systematic review and meta-analysis. J. Commun. Disord. 85, 105992 (2020).
- Seager, E., Sampson, S., Sin, J., Pagnamenta, E. & Stojanovik, V. A systematic review of speech, language and communication interventions for children with Down syndrome from 0 to 6 years. Int. J. Lang. Commun. Disord. 57, 441–463 (2022).
- Nielsen, M., Haun, D., Kärtner, J. & Legare, C. H. The persistent sampling bias in developmental psychology: A call to action. J. Exp. Child Psychol. 162, 31–38 (2017).
- Scheidecker, G. et al. Ending epistemic exclusion: toward a truly global science and practice of early childhood development. Lancet Child Adolesc. Health 8, 3–5 (2024).
- Qi, P., Zhang, Y., Zhang, Y., Bolton, J. & Manning, C. D. Stanza: A Python Natural Language Processing Toolkit for Many Human Languages. Preprint at https://doi.org/10.48550/arXiv.2003.07082 (2020).
- Qi, P., Dozat, T., Zhang, Y. & Manning, C. D. Universal Dependency Parsing from Scratch. in Proceedings of the CoNLL 2018 Shared Task: Multilingual Parsing from Raw Text to Universal Dependencies (eds. Zeman, D. & Hajič, J.) 160–170 (Association for Computational Linguistics, Brussels, Belgium, 2018). doi:10.18653/v1/K18-2016.
- Miller, J. F., Sedey, A. L. & Miolo, G. Validity of Parent Report Measures of Vocabulary Development for Children With Down Syndrome. J. Speech Lang. Hear. Res. 38, 1037–1044 (1995).
- Berglund, E., Eriksson, M. & Johansson, I. Parental Reports of Spoken Language Skills in Children With Down Syndrome. J. Speech Lang. Hear. Res. 44, 179–191 (2001).
- Galeote, M., Checa, E., Sánchez-Palacios, C., Sebastián, E. & Soto, P. Adaptation of the MacArthur-Bates Communicative Development Inventories for Spanish Children With Down Syndrome: Validity and Reliability Data for Vocabulary. Am. J. Speech Lang. Pathol. 25, 371–380 (2016).
- Sutton, R. S. & Barto, A. G. Reinforcement Learning: An Introduction, 2nd Ed. xxii, 526 (The MIT Press, Cambridge, MA, US, 2018).
- Memarian, B. & Doleck, T. A scoping review of reinforcement learning in education. Comput. Educ. Open 6, 100175 (2024).
- Eldan, R. & Li, Y. TinyStories: How Small Can Language Models Be and Still Speak Coherent English? Preprint at https://doi.org/10.48550/arXiv.2305.07759 (2023).
- Abdin, M. et al. Phi-3 Technical Report: A Highly Capable Language Model Locally on Your Phone. Preprint at https://doi.org/10.48550/arXiv.2404.14219 (2024).

