Electropalatography in the assessment and treatment of speech difficulties in children with Down syndrome
Many children with Down syndrome experience significant speech difficulties which in turn affects their speech intelligibility. This paper describes how electropalatography, a computer-based technique which uses visual feedback to alter speech production, is being used at Queen Margaret University, to assess and treat speech difficulties in a group of children and young people with Down syndrome. Encouraging results from a single case are reported.
Wood, S. (2010) Electropalatography in the assessment and treatment of speech difficulties in children with Down syndrome. Down Syndrome Research and Practice, 12(2), 98-102. doi:10.3104/reports.2093
It has been well documented in the literature that individuals with Down syndrome demonstrate difficulties with speech production and often present with reduced intelligibility. Many studies have suggested that the difficulties are characterised by a delay in phonological development [1-5] . Stoel -Gammon summarized the processes used by children with Down syndrome as cluster reduction, final consonant deletion, stopping of fricatives, pre-vocalic voicing, word initial gliding, word final vocalization, and devoicing of word final obstruents [6] . Others have suggested that a purely phonological delay is an over-simplistic view and that many people with Down syndrome also show developmental differences such as greater variability in production [7] and unsystematic replacement of final voiceless fricatives by other voiceless fricatives [4] . Roberts et al., who collected data from 32 boys with Down syndrome aged 4 to 13 years, found additional systematic errors not previously reported, for example palatal fronting, fricative simplification, deaffrication, and lateralisation of sibilants [8] . In addition to phonological processes researchers are beginning to suggest that children with Down syndrome may be demonstrating characteristics synonymous with a diagnosis of apraxia of speech [9,10] .
It is generally accepted that the speech problems associated with Down syndrome often lead to decreased intelligibility [10] . In a survey of 937 parents of children with Down syndrome over 95% of parents reported difficulties understanding their child by individuals immediately outside the family [11] . Buckley and Sacks reported that over half the adolescent girls and approximately 80% of boys in their survey were rated as unintelligible to strangers [12] .
Early studies identifying speech errors have been based on subjective judgments by trained listeners. Although valuable for many assessment purposes, such judgments can be highly unreliable [13,14] and give no precise objective information on activities of individual speech organs. Kumin states "there have not been adequate descriptions of the oral motor difficulties. There also have not been studies of various treatment approaches for oral motor difficulties and their results" [10: p.12] . Such information is vital if we are to obtain greater understanding of the speech motor control characteristics of children with Down syndrome. Hamilton goes as far as to claim that until rigorous objective assessments underpin precise diagnoses of their speech problems, interventions offered to children with Down syndrome are unlikely to be effective [15] .
The few instrumental studies of speech characteristics of children with Down syndrome have provided additional qualitative and quantitative speech production data such as undershoot of target articulations, abnormal patterns of lingual palatal contact, longer closure durations, longer transition times between consonants in cluster, slower DDK rates, etc. [15,16] . These studies have been based on very small numbers of individuals with Down syndrome (3 adolescents and one 10-year old respectively).
A 3 year project funded by the Medical Research Council using electropalatography (EPG) to investigate impaired motor speech control in children with Down syndrome is nearing completion in Edinburgh. EPG is a non-invasive technique which visually displays the timing and movement of the tongue's contact with the hard palate during continuous speech. It requires the individual to have a custom made artificial palate (Figure 1) which fits snugly against the roof of the mouth. Embedded into the artificial palate are 62 electrodes that register when the tongue is touching them. An individual's articulation can be compared to standard patterns for English consonants (see examples in Figure 2) and error patterns noted. EPG gives objective and detailed analysis of the articulation and may identify errors which cannot be detected by perceptual analysis alone (e.g. double articulations).
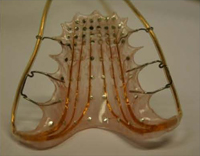
Figure 1 | EPG palate
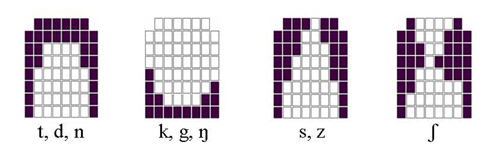
Figure 2 | Standard articulatory patterns for lingual consonants
EPG can also be used to modify articulatory patterns by using visual feedback. A target articulation pattern characteristic of a particular sound is displayed on a computer screen and during a therapy session the child attempts to copy this correct articulation by monitoring their own contact patterns in real time (see Figure 3).The technique is particularly suited for children with Down syndrome for a number of reasons. First, the link between the speech movements and the visual display is a direct and conceptually very simple one. Second, by utilising visual feedback, EPG is particularly suited to individuals with Down syndrome whose visual processing skills are described as a relative strength.
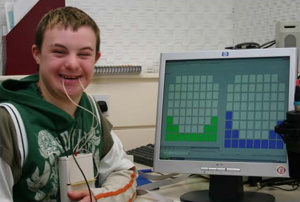
Figure 3 | Child during therapy session. The target articulation is displayed on the right hand side of the computer screen. The left hand side shows the individual's successful attempt to match the target articulation.
The aim of the project is to gain a greater understanding of the speech motor control deficiencies associated with Down syndrome and how these are likely to impact on speech development. The longer term aim is to apply this knowledge therapeutically to develop speech production skills and thus enhance the quality of life.
Twenty-seven children with Down syndrome were recruited to take part in the project. Following detailed testing on speech, language and cognitive assessments the participants were randomly assigned to one of 3 groups. Nine children received EPG visual feedback therapy, 9 received traditional articulation therapy (i.e. not using EPG) and 9 received no treatment within this study but continued therapy as usual with their regular speech and language therapist. Treatment consisted of 24 sessions of therapy. All 27 participants with Down syndrome were reassessed using EPG immediately following therapy (or 3 months later for the no therapy group) and 3 and 6 months post therapy to monitor progress made in therapy and further change.
Detailed EPG analysis is ongoing. So far we can report a wide range of speech skills in children with Down syndrome who demonstrate both developmental and disordered error patterns. The majority of the children are highly unintelligible in conversation. EPG has revealed a number of additional errors which cannot be detected through a purely perceptual-based analysis. For example, weak articulations (where there are fewer EPG contacts than is expected), increased variability of articulation when compared to typically developing children and sequencing difficulties.
Assessment and therapy results from one child will be illustrated to highlight some of the errors and the improvements that are being seen from EPG therapy. This 11 year old girl with Down syndrome had a verbal age equivalent of 4.08 years and a performance age equivalent of 6.04 years based on results from the WPPSI-IIIUK. Assessment of language skills using the CELF-PUK suggested a receptive language age equivalent of 3 years 11 months and an expressive language age equivalent of 3.00 years. Analysis of the DEAP (Diagnostic Evaluation of Articulation and Phonology) revealed 57% of consonants were accurately produced which equated to an age equivalent of 3 years. Errors were summarized as follows: distorted and inconsistent productions of fricatives and affricates; voicing errors; weak syllable deletion; and cluster reduction. Analysis of the EPG data confirmed that fricatives and affricates were distorted and therapy focussed on remediating the production of /s/ and /ʃ/. Only production of /s/ will be reported here. Figure 4 shows variation in the production of word initial /s/ for "sun". This girl had a variability index of 16.77 which contrasts with 7.04 for children matched for cognitive ability.
Following 24 therapy sessions the child underwent reassessment. This revealed an increase of consonants correct (PCC) as measured by the DEAP from 57% to 87% with a corresponding increase in age equivalence to 4 years. She demonstrated more consistent correct production of both /s/ and /ʃ/ with a variability score of 9.68 (see Figure 5). Cluster reduction remained a feature of her speech as did weak syllable deletion.
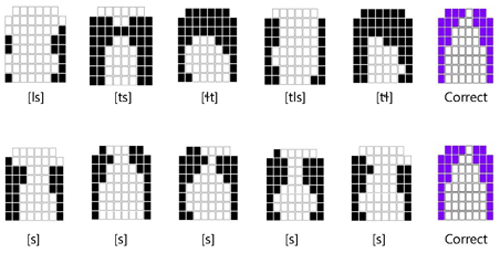
Figure 4 (top) | Five examples of the target /s/ in "sun" spoken by the same child with Down syndrome before therapy showing increased variability. Correct production is given on the far right.
Figure 5 (below) | Five repetitions of the target /s/ in "sun". The EPG patterns demonstrate accurate and consistent lingual palatal contact patterns immediately post therapy.
This girl made excellent progress during 24 therapy sessions (12 weeks). Towards the end of therapy she was able to achieve correct placement for /s/ in single words and sentences and was able to carryover this skill within the therapeutic context, using /s/ correctly in phrases without EPG feedback. PCC had increased from 57% to 87% representing an improvement in all sibilants, not just in her production of /s/ and variability decreased, perhaps indicating improved motor control although this still remains higher than typically developing children. She continues to present with intelligibility issues but many are related to speech rate and voice.
References
- Dodd B, Leahy J. Phonological disorders and mental handicaps. In: Beveridge M and Conti-Ramsden G, editors. Language and Communication in Mentally Handicapped People. London: Chapman and Hall;1989.
- Shriberg LD, Widder CJ. Speech and prosody characteristics of adults with mental retardation. Journal of Speech and Hearing Research. 1990;33:627-653.
- Rosin M, Swift E, Bless D, Vetter DK. Communication profiles of adolescents with Down syndrome. Journal of Childhood Communication Disorders. 1998;12:49-64.
- Stoel-Gammon C. Phonological analysis of four Down's syndrome children. Applied Psycholinguistics. 1980;1:31-48.
- Stoel-Gammon C. Phonological development in Down syndrome. Mental Retardation and Developmental Disabilities Research Reviews. 1997;3:300-306.
- Stoel-Gammon C. Down syndrome phonology: Developmental patterns and intervention strategies. Down Syndrome Research and Practice. 2001;7(3):93-100. [Read Online] doi:10.3104/reviews.118
- Dodd B. A comparison of the phonological systems of mental age matched normal, severely subnormal and Down's syndrome children. British Journal of Disorders of Communication. 1976;11:27-42.
- Roberts J, Long SH, Malkin C, Barnes E, Skinner M, Hennon EA, Anderson K. A comparison of phonological skills of boys with Fragile X syndrome and Down syndrome. Journal of Speech, Language and Hearing Research. 2005;48:980-995.
- Kumin L, Adams J. Developmental apraxia of speech and intelligibility in children with Down syndrome. Down Syndrome Quarterly. 2000;5(3):1-7.
- Kumin L. Speech intelligibility and childhood verbal apraxia in children with Down syndrome. Down Syndrome Research and Practice. 2006;10(1):10-22. [Read Online] doi:10.3104/reports.301
- Kumin L. Intelligibility in speech in children with Down syndrome: Parents' perspective. Perceptual and Motor Skills. 1994;78:307-313.
- Buckley SJ, Sacks BI. The Adolescent with Down Syndrome: Life for the Teenager and Family. Portsmouth, England: Portsmouth Polytechnic Institute;1987.
- Kent RD. Hearing and believing: Some limits to the auditory-perceptual assessment of speech and voice disorders. American Journal of Speech-Language Pathology. 1996:5:7-23.
- Santelmann L, Sussman J, Chapman K. Perception of middorsum palatal stops from the speech of three children with repaired cleft palate. Cleft Palate Craniofacial Journal. 1999;36:232-242.
- Hamilton C. Investigation of the articulatory patterns of young adults with Down's syndrome using electropalatography. Down Syndrome Research and Practice. 1993;1(1):15-28. [Read Online] doi:10.3104/reports.7
- Gibbon FE, McNeill AM, Wood SE, Watson JMM. Changes in linguapalatal contact patterns during therapy for velar fronting in a 10-year-old with Down's syndrome. International Journal of Communication Disorders. 2003;38(1):47-64.
Acknowledgements
Thank you to all of the children and young people taking part in this study, and their families. Grateful thanks to Down's Syndrome Scotland and to NHS colleagues for their help in recruiting to this study. Thanks are extended to Ann Robertson for administering the cognitive assessments. This research was funded by the UK Medical Research Council (project grant no. G0401388).
Received: 04 March 2008; Accepted: 11 March 2008; Published online: January 2010

