Responsive Teaching: Early intervention for children with Down syndrome and other disabilities
Responsive Teaching is an early intervention curriculum designed to address the cognitive, language, and social emotional needs of young children with developmental problems. This innovative intervention model was derived from research conducted primarily with children with Down syndrome and their mothers. Results from these studies indicated that during the early childhood years, parents promote their children's development by engaging in highly responsive interactions throughout their daily routines. The effects of responsiveness are mediated by the impact it has on children's use of several pivotal developmental behaviors, such as social play, attention, initiation and persistence. Responsive Teaching helps parents learn to use Responsive Teaching strategies to promote the pivotal developmental behaviors that are relevant to their children's developmental needs. Research with 50 children with developmental problems and their parents indicated that Responsive Teaching was highly effective at addressing children's developmental and social emotional needs. The effects of this intervention were mediated by the impact that RT strategies had on children's pivotal developmental behaviors.
Mahoney, G, Perales, F, Wiggers, B, and Bob Herman, B. (2006) Responsive Teaching: Early intervention for children with Down syndrome and other disabilities. Down Syndrome Research and Practice, 11(1), 18-28. doi:10.3104/perspectives.311
Responsive Teaching (RT) (Mahoney & MacDonald, 2007) is a child development early intervention curriculum that was designed to be implemented by parents and other caregivers who spend significant amounts of time interacting with and caring for young children. RT was developed to help adults maximize the potential of each of their routine interactions with their children so that they support and enhance children's development and well being. This curriculum encourages children to develop and use the 'pivotal behaviors' that are the foundations for developmental learning, such as social play, initiation, problem solving, joint attention, conversation, trust, cooperation, persistence and feelings of competence. The instructional strategies that are at the heart of Responsive Teaching are 'easy to remember' suggestions that adults can incorporate into daily routines with children.
Responsive Teaching is designed to promote three domains of developmental functioning. These include the following:
- Cognition - children's ability to think, reason, solve problems and learn new information about their world and relationships;
- Communication - children's ability to convey their feelings, observations and intentions and respond to the feelings, observations and intentions of others through nonverbal, symbolic and spoken language;
- Social-emotional functioning - children's ability to engage in and enjoy developmentally appropriate interactions with parents, adults and other children as well as to comply with reasonable rules and expectations.
In this paper we will discuss four issues related to Responsive Teaching. First we will describe the research findings conducted mostly with children with Down syndrome that provided the empirical foundations for the design of this curriculum. Second, we will describe the procedures for implementing this intervention. Third we will describe the results of a one year study of the effectiveness of Responsive Teaching that was conducted with 50 children who had developmental problems or delays. Finally, we will discuss the implications that this curriculum has for early intervention practice.
Empirical foundations for Responsive Teaching
How do parents influence children's development?
In the 1980s, Mahoney and his colleagues initiated a series of studies designed to determine how parents influenced the rate of development of their young children with developmental disabilities. The sample for these studies included 60 mother-child pairs in which 90% of the children had Down syndrome and the remaining children had conditions such as Williams' Syndrome and hydrocephaly. The sample included twenty children each at the 12- 24- and 36- month age range. For the entire sample, children's average chronological age was 24.7 months and their average Bayley Developmental Age (Bayley, 1969) was 13.9 months.
The first study (Mahoney, Fingers & Powell, 1985) assessed the relationship of mothers' style of interacting with their children to children's rate of developmental progress as measured by the Bayley Scales of Mental Development (Bayley, 1969). Mothers were videotaped while they played with their children in their homes with a set of developmentally appropriate toys. The first 10 minutes of these videotapes was coded with a global rating scale referred to as the Maternal Behavior Rating Scale (Mahoney, Powell & Fingers, 1986). The 18 items on this scale assessed three dimensions of mothers' interactive style. These included responsiveness or child orientation, quantity of stimulation, and directiveness or performance orientation. Responsiveness/child orientation included items such as sensitivity, responsiveness, reciprocity, enjoyment and playfulness. Quantity of stimulation included items that assessed how much social, physical and verbal stimulation mothers provided their children. Directiveness or performance orientation included how much mothers attempted to teach or direct their children's play.
Results from this study indicated that the way mothers interacted with their children accounted for almost 25% of the variability in children's rate of development. Whether children were 12, 24 or 36 months of age, the children who had the highest rates of development were the children whose mothers were high in responsiveness or child-orientation, and low in behaviors that involved directing their child's play and teaching their child (Mahoney, Fingers & Powell, 1985). These results suggested that if mothers provided high levels of verbal and physical stimulation and attempted to teach their children developmental behaviors by guiding and directing them, their children had lower Bayley Developmental Scores compared with the other children who were at their same age level. However, if mothers engaged interactions in which they focused on enjoying and having fun with their children and in which they responded to their children by encouraging and supporting the behaviors that they were initiating on their own, their children had higher Bayley Developmental Scores.
The next two studies were conducted to determine if the way mothers communicated with their children was related to their children's rate of communication development (Mahoney, 1988a, b). The same observations of parent-child interaction as used in the preceding study were also used for these studies. Each of the verbal and nonverbal communications that took place between mothers and their children during the full 20 minute observation was transcribed. The structure, complexity and pragmatic function of each of these utterances were then coded. The manner that mothers and children responded to each others' communicative attempts was also coded.
Results indicated that there were no significant correlations between the structure and pragmatic functions of mothers' communication with children's rate of development and level of communication functioning. These findings suggested that the content and complexity of mothers' conversations with children were not related to the rate that children were developing their language and communications skills. However, the way mothers responded to their children's communication attempts was strongly associated with children's level of communication functioning.
Mothers' responsiveness to their children's communication was classified into one of three general patterns. One group of mothers, called Responders, was highly responsive to their children's verbal and nonverbal attempts to communicate. These mothers treated their children's attempts to communicate as legitimate communications, even if their children's vocalizations or gestures had no obvious meaning or their intentions were unclear. Responders' communications tended to be focused on their children's conversational topics or play interests. The second group of mothers, called Attenders, was highly attentive to their children, but did not respond frequently to the communications their children initiated. They communicated a great deal with their children, but their communications were focused on providing information (e.g., names, colors, functions of objects) or asking their children to answer questions that were often not related to what children were currently interested in communicating about. The third group, called Ignorers, was very inattentive to their children's communication. While they did speak to their children, they either ignored or failed to pay attention to most of their children's communication attempts.
The children of these three groups of mothers had very different levels of communication functioning. Their rate of language development was assessed with the REEL (Receptive and Expressive Emergent Language Scale) (Bzoch & League, 1970). Children of Responders had higher language age scores (M Language Age = 15.3 months) than children of Attenders (M Language Age =12.7 months) who in turn had higher language age scores than children of Ignorers (M Language Age =11.6 months). The differences between these three groups of children were also reflected in their communication with their mothers, including their frequency of vocal and communicative behaviors, percentage of spontaneous and elicited imitation, use of words, and number of meaningful nonverbal communications (Mahoney, 1988b).
Overall, results from these three studies suggest that parents promote their children's cognitive and communication development primarily by engaging in highly responsive interactions with them. While similar findings had been reported with children who do not have disabilities prior to these findings (e.g., Ainsworth & Bell, 1975; Elardo, Bradley & Caldwell, 1975; Stern et al., 1969; Lewis & Goldberg, 1969), this research was the first to document this effect with children with Down syndrome and other disabilities. These findings were provocative because they contradicted the prevailing methodologies that were being used in early cognitive and language interventions (Bailey & Wolery, 1984), many of which are still being used today (e.g., Guralnick, 1997). At the time that these results were published, the majority of early intervention professionals were using highly directive instructional procedures such as modelling, shaping, elicited imitation, prompting and extrinsic reinforcement to teach cognitive and communication skills to children with disabilities. Professionals who worked collaboratively with parents were recommending that parents also use directive instructional procedures with their children at home, which was clearly in conflict with these research findings.
How does responsiveness promote children's learning and development?
In contemporary early intervention practice, intervention objectives consist of the developmental behaviors and concepts that children have not yet mastered (Lynch & Beare, 1990; Pretti-Frontczak & Bricker, 2000; Weisenfeld, 1986). This is based upon the idea that children who have developmental problems or delays will 'catch up' as they learn and use these higher level developmental skills. Directive instructional procedures must be used to help children perform and learn the skills that have been targeted as their intervention objectives, since children are unlikely to engage in these behaviors on their own.
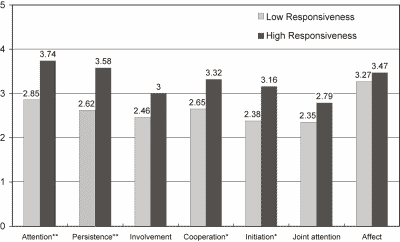
Figure 1 | The relationship between mothers' to children's global pivotal
This study included 45 infants and toddlers with developmental disabilities who were 25 months old and had a variety of developmental problems (Mahoney, Kim & Lin, in press). These children were divided into two groups: children of High Responsive Mothers (n=28) and children of Low Responsive Mothers (n=17) based upon ratings of how mothers interacted with their children using the Maternal Behavior Rating Scale (Mahoney, 1999). The manner in which these children interacted with their mothers was then measured using the Child Behavior Rating Scale (CBRS: Mahoney & Wheeden, 1998). As illustrated on Figure 1, children of High Responsive mothers had higher ratings on each of the seven CBRS items than did children of Low Responsive Mothers.
These findings suggest that, although responsive interaction may not be effective at teaching higher level developmental skills or concepts, it may be highly effective at teaching a different, but perhaps more critical, class of developmental behaviors. Most of the behaviors measured by the CBRS are considered by child development experts to be the processes or patterns of behavior that children themselves must demonstrate in order to learn. Specifically, the amount children learn from a particular activity or experience is largely dependent on how actively they are engaged in the activity. Many of the 'behaviors' that are assessed by the Child Behavior Rating Scale reflect the critical behavioral processes that children utilize to initiate and maintain active engagement in activities.
To test the idea that children's developmental learning is influenced by the amount they engage in the behaviors measured by the CBRS, the 45 infants and toddlers described above were divided into two groups, High Engagers and Low Engagers. High Engagers had average CBRS scores that were above the midpoint, while Low Engagers had scores that were at the midpoint or lower. The average developmental age scores of these children was then compared on two developmental measures, the Vineland Adaptive Behavior Scale (Sparrow, Balla & Cicchetti, 1984) and the Transdisciplinary Play based Assessment (Linder, 1993). As illustrated on Figure 2, across the nine developmental subscales from these two assessments, when differences in children's age were controlled, children who were High Engagers had significantly higher developmental age scores than children who were Low Engagers.
These results suggest that the behaviors parents encourage when they interact responsively with their children are the learning processes that are the foundations for developmental learning. Following the work of Koegel and his colleagues (Koegel, Koegel & Carter, 1999), we refer to these as pivotal behaviors. That is, the child behaviors that parents promote by interacting responsively are pivotal to wide areas of functioning such that improvements in these behaviors enhance children's ability to learn the skills and concepts that are the foundations for higher levels of developmental functioning.
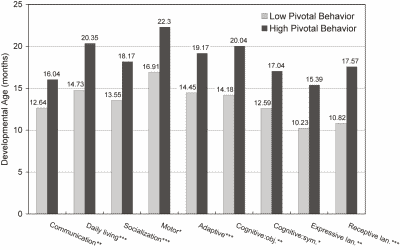
Figure 2 | The relationship of children's pivotal behavior level to their child development ages
Based upon the empirical research findings reported above, the Responsive Teaching curriculum was organized around the idea that responsive parents promote children's development more by encouraging children to engage in pivotal developmental behaviors and less by directly teaching the skills and concepts that are the benchmarks of higher levels of functioning. The more responsively parents interact with their children, the more they prompt their children to use these pivotal behaviors. Parents who consistently engage in a responsive style of interacting with their children in the multitude of interactive episodes they have each day help their children to develop habits of using these pivotal behaviors or learning processes. Over time this helps to maximize children's development and social-emotional well-being.
Implementing Responsive Teaching
The Responsive Teaching curriculum includes 66 Responsive Teaching strategies and 16 Pivotal Behaviors that are targeted as developmental intervention objectives. Responsive Teaching Strategies are brief, easy-to-remember suggestions that parents can use to use to monitor and change how they interact with their children at any time and in any situation. These strategies, which are listed in Table 1, are designed to help parents incorporate the five interactive dimensions that are associated with responsiveness into their own interactions with their children. These dimensions include the following:
- Reciprocity - frequent episodes of interaction that are characterised by a balanced, 'give and take' relationship;
- Contingency - interactions that have an immediate and direct relationship to a child's previous behaviors that support and encourage the child's actions, intentions, and communications;
- Shared Control - guidance and direction that facilitates and expands the actions and communications which the child initiates or leads;
- Affect - expressive, animated and warm interactions that are characterised by enjoyment or delight in interacting with the child;
- Match - interactions and requests that are adjusted to the child's developmental level, current interests, and behavioral style or temperament.
| RECIPROCITY | |
|---|---|
| Engagement | Be physically available and interactive |
| Play frequently together | |
| Get into my child's world | |
| Use mirroring and parallel play to join an activity | |
| Expect my child to interact | |
| Balance | Take one turn and wait |
| Keep my child for one more turn than usual | |
| Play with sounds back and forth | |
| Get from my child as much as I give to him | |
| Communicate less so my child communicates more | |
| Joint Action Routines | Play face-to-face games without toys |
| Sustain repetitive play or action sequences | |
| Join perseverative play (make it interactive) | |
| Play with my child with toys | |
| Make a habit of communicating during joint activity routines | |
| CONTINGENCY | |
| Awareness | Observe my child's behavior |
| Take my child's perspective | |
| Be sensitive to my child's state | |
| Timing | Respond quickly to my child's signals, cries or nonverbal requests |
| Respond immediately to little behaviors | |
| Discipline promptly and comfort | |
| Intent | Respond to unintentional vocalizations, facial displays and gestures "as if" they were meaningful conversation |
| Accept incorrect word choice, pronunciation approximations by responding to my child's intention or word | |
| Translate my child's actions, feelings, intentions into words | |
| Rephrase unclear vocalizations and word approximations with words that match my child's actions or intentions | |
| Interpret noncompliance as a choice or lack of ability | |
| Frequency | Explore how responsive strategies can be used to enhance my child's participation throughout daily routines |
| Encourage multiple caregivers to use responsive strategies | |
| CONTROL | |
| Moderate Direction | Communicate without asking questions |
| Imitate my child's actions and communications | |
| Give my child frequent opportunities to make choices | |
| Facilitation | Expand to show my child the next developmental step |
| Expand to clarify my child's intention or develop my child's topic | |
| Wait silently for a more mature response | |
| Play for a purpose | |
| Change the environment | |
| AFFECT | |
|---|---|
| Animation | Be animated |
| Wait with anticipation | |
| Respond to my child in playful ways | |
| Be more interesting than my child's distractions | |
| Accompany communication with intonation, pointing and nonverbal gestures | |
| Enjoyment | Act as a playful partner |
| Interact for fun | |
| Turn routines into games | |
| Repeat activities my child enjoys | |
| Warmth | Be physical but gentle |
| Respond affectionately to my child's cries and needs for attention | |
| Comfort my child when fussy, irritable or angry | |
| Acceptance | Value what my child is doing |
| Treat my child's fears as meaningful and legitimate | |
| Accept whatever my child does | |
| Talk about the novel, funny and good things my child is doing | |
| MATCH | |
| Developmental Match | Interpret my child's behavior developmentally |
| Know the developmental skills my child seems ready to learn | |
| Request actions that match my child's developmental level | |
| Act in ways my child can do | |
| Communicate the way my child communicates | |
| Have developmentally appropriate rules and expectations | |
| Interest Match | Read my child's behavior as an indicator of interest |
| Follow my child's focus of attention | |
| Follow my child's lead | |
| Behavioral Style Match | Be sensitive to my child's sensations |
| Observe how my child ordinarily engages in interaction | |
| Respond to my child's behavioral state | |
| Have expectations that conform to my child's behavioral style | |
Table 1 | Responsive Teaching Strategies.
Responsive Teaching Strategies are based upon the principle of 'active learning'. They help parents engage in responsive interaction before this is their routine style of interacting with their children. As parents use RT strategies, many discover the impact responsiveness has on their children's engagement and participation. These experiences help parents appreciate the implications this style of interaction has for all encounters with their children. It motivates them to incorporate RT strategies into their spontaneous interactions, and eventually results in their instinctively using a responsive style of interacting with their children.
Pivotal Behaviors are a small set of developmental processes that children use to learn developmental skills and competencies across the three developmental domains of cognition, communication and social emotional functioning. The pivotal behaviors included in Responsive Teaching were identified from contemporary theory and research in child development, including constructivist theories of cognitive development (Piaget, 1963; Vygotsky, 1978), communication theories of language development (Bates, Benigni, Bretherton, Camioni & Volterra, 1979; Bruner, 1975, 1983), and developmental theories of social-emotional development (Bowlby, 1969; Goleman, 1995). They are the developmental behaviors that parents and others promote by engaging in responsive interaction. Responsive Teaching targets the 16 pivotal behaviors listed in Table 2 as the intervention objectives that are used to address children's developmental needs.
For each pivotal behavior included in Responsive Teaching, there are 6 to 10 sets of Discussion Points. These describe in simple language the theories of development that are the basis for this curriculum. They explain how the pivotal behavior that has been targeted as the intervention objective will both improve children's developmental learning and help parents attain the outcome they want for their child. Discussion Points have been designed so that parents can complete each intervention session having a few clearly defined ideas to think about that support the RT strategies that they have been asked to use with their children. Discussion Points formalise what good professionals typically do. They provide a focused and cohesive structure for providing child development information to parents.
RT Intervention sessions can be conducted individually with parents and their children either in homes or center-based settings, or with groups of parents whose children have similar developmental concerns. Each session focuses on one or two pivotal behaviors that are relevant to the needs of the child. For each pivotal behavior, the interventionist introduces one or two sets of Discussion Points to provide parents with background information about the pivotal behaviors they are being asked to encourage their children to use throughout the daily routine. Sessions also help parents to learn and use one or two RT strategies which the curriculum recommends for promoting the pivotal behaviors being targeted. In addition, when pivotal behaviors are first introduced, and periodically thereafter, parents and professionals assess the child's use of the pivotal behavior being targeted with the Pivotal Behavior Rating Scale. This assessment tool provides objective criteria for assessing children's progress on their intervention objectives.
RT does not prescribe a fixed sequence of activities for addressing pivotal behaviors. Rather it is a menu driven curriculum that provides interventionists the flexibility of choosing intervention objectives, RT strategies and Discussion Points that are best suited both to the developmental needs of children and to the learning pace and style of parents. RT sessions can last from 30 minutes to one hour. Typically sessions are provided on a weekly basis to give parents the time they need to try to use and explore the information presented in each session. However, there is no evidence that different levels of intensity of RT sessions would be more or less effective. Responsive Teaching has also been designed so that parents can implement it with their children on their own.
| DEVELOPMENTAL DOMAINS | COGNITION | COMMUNICATION/LANGUAGE | SOCIAL/ EMOTIONAL |
|---|---|---|---|
| Pivotal Behaviors | Social Play | Joint Activity | Trust |
| Initiation | Joint Attention | Empathy | |
| Exploration | Vocalisation | Cooperation | |
| Practice | Intentional Communication | Self Regulation | |
| Problem Solving | Conversation | Feelings of Control | |
| Feelings of Confidence |
Table 2 | Responsive Teaching Pivotal Behaviors.
The effectiveness of Responsive Teaching
Recently Mahoney and Perales (2005) reported results from a one year evaluation of the children and parents who were involved in the development of the Responsive Teaching curriculum. This evaluation examined whether children who received Responsive Teaching made significant developmental and social emotional improvements, and whether the improvements they achieved in this program were related to either their parents' learning to interact more responsively (e.g., reciprocity, contingency, shared control, affect and match) and/or to improvements in children's use of pivotal behaviors.
Fifty mother-child pairs participated in this evaluation. The children's ages ranged from 12 to 54 months, with 85% of the children being younger than 36 months when they began. The average age of the mothers was 32.6 years and most were Caucasian (89.1%) and married (92.7%). The sample included 20 children with Autism Spectrum Disorders (ASD) and 30 children with Developmental Disorders (DD). All of these children had significant delays in cognition and/or communication. While children with DD (Mean age = 23.3 months) were younger than children with ASD (Mean age = 32.4 months), the developmental ages for these two groups were nearly the same.
Subjects received RT during weekly one hour parent-child sessions. They received an average of 33 sessions over a one year period of time. A comprehensive child development assessment was conducted at the beginning and end of intervention to evaluate the effects of this intervention. The Transdisciplinary Play Based Assessment (TPBA, Linder, 1993) was used to assess children's cognitive and language development. The Temperament and Atypical Behavior Scale (TABS) (Bagnato, Neisworth, Salvia & Hunt, 1999) and the Infant Toddler Social Emotional Assessment (Carter & Briggs-Gowan, 2000) were used to assess children social-emotional functioning.
Mothers' style of interaction and children's pivotal behavior were also assessed from a seven minute videotaped observation of children and mothers playing together. A modified version of the Maternal Behavior Rating Scale (Mahoney, 1999) was used to assess mothers' style of interacting with their children, and the Child Behavior Rating Scale (Mahoney & Wheeden, 1998) was used to assess children's pivotal behavior.
As expected, pre- post comparisons indicated that the Responsive Teaching strategies helped mothers make significant increases in their levels of Responsiveness and Affect while interacting with their children. In addition, over the course of intervention, children made improvements in all seven of the pivotal behaviors assessed by the Children's Behavior Rating Scale.
To assess intervention effects on children's cognitive and language development a proportional change index (PCI) was computed. PCIs compare children's rate of development during intervention to their rate of development before intervention. PCIs indicated that children's rate of development during intervention was 123% greater than it was before intervention. Specifically, children made a 64% increase in their rate of cognitive development, a 167% increase in their rate of expressive language development and a 138% increase in their receptive language development.
Children with DD did not have social emotional problems at the beginning of intervention as indicated by their TABS scores, and made little improvement in this domain during intervention. However, children with ASD made a 36% improvement in their overall scale score from the TABS. This was evident on three TABS subscales, detached, under-reactivity, self regulation. Similarly, on the ITSEA the scale scores for children with ASD improved by 15% in Self Regulation and 20% in Social Competence.
To determine whether Responsive Teaching was truly responsible for these developmental improvements, analyzes were conducted to examine if the changes in mothers' responsiveness and children's pivotal behavior that were promoted through Responsive Teaching were related to the developmental and social emotional improvements that children made. If the children who made the greatest improvements were the ones whose mothers' changes in responsiveness resulted in the improvements in their pivotal behavior, then there would be a strong reason to believe that Responsive Teaching is a highly effective developmental intervention curriculum (Shadish, Cook & Campbell, 2002).
Results from these analyzes produced the following findings. First, the changes in mothers' responsiveness during intervention accounted for 20% of the variance in changes in children's pivotal behavior. These findings indicate that there was a linear relationship between the degree to which mothers changed their level of responsiveness with changes in children's pivotal behavior. When mothers did not change their responsiveness, children made negligible increases in their pivotal behaviors. However, when mothers became more responsive, the degree that children increased their pivotal behavior was directly related to the degree to which parents changed their responsiveness. The more responsive mothers became during intervention, the more children increased their pivotal behavior.
Second, changes in children's pivotal behavior accounted for an average of 10% of the variance in improvements in children's rate of development for each developmental domain. In other words, how much children's pivotal behavior changed during intervention was related to the improvements in their Developmental Ages. Children who did not change their pivotal behavior attained developmental age scores that were comparable to their expected Developmental Age scores. However, children who increased their pivotal behavior attained Developmental Ages that were greater than their Expected Developmental Ages.
Third, analyzes were conducted to examine how changes in children's pivotal behavior contributed to changes in their social-emotional functioning. Results indicated that changes in children's pivotal behavior were not related to their social emotional improvements. Nonetheless, when we divided the sample into children who did not change their pivotal behaviors during intervention (No Change, n = 13) versus children who made at least some changes (Change, n =34), children in the Change Group made improvements on four of the five TABS subscales that were at least 100% greater than improvements made by the No Change Group.
Results from this evaluation indicated that children made remarkable developmental and social emotional improvements when their parents used Responsive Teaching with them. The magnitude of developmental improvements that we observed is comparable to, and in most cases far greater than, the level of improvements that have been reported for most other early intervention procedures (c.f., Guralnick, 1997). While there was no Control group, the analyzes that were conducted suggested that the effects of treatment were causally related to Responsive Teaching. Approximately one third of the parents who participated in this project were not very successful in using RT strategies. This was indicated by the fact that the RT strategies had no impact on these mothers' level of responsiveness with their children. Children of these mothers made no improvements in either their pivotal behavior or in their development or social emotional functioning during intervention. However, for the remaining two-thirds of the sample, the picture was just the opposite. RT strategies were effective at helping these mothers learn to interact more responsively with their children. How much these mothers improved their responsiveness was related both to increases in their children's pivotal behavior and to improvements in their children's developmental and social-emotional well-being.
Implications of Responsive Teaching for parents of children with Down syndrome
There are several important implications that Responsive Teaching has for children with Down syndrome and their parents. First, it is important to note that children with Down syndrome and their parents were the starting point for developing this curriculum. As explained earlier in this paper, the process of developing the intervention procedures that are now known as Responsive Teaching were initiated because of research findings which suggested that parental responsiveness played a major role in fostering the cognitive and communication functioning of young children with Down syndrome.
Although only one child with Down syndrome was included in the Responsive Teaching evaluation sample, the overall results of the evaluation suggested that RT can improve the developmental status of children with a wide range of disabilities. The child with Down syndrome who participated in the Responsive Teaching evaluation made developmental gains that were comparable to the other children in our sample. This child made a 113% improvement across all developmental domains and a 145% improvement in his rate of language development. While these results are encouraging, clearly they are not sufficient for claiming that Responsive Teaching is an effective intervention for these children. To make this claim, Responsive Teaching would need to be validated with a larger, more representative sample of children with Down syndrome, and intervention outcomes would need to be examined for more than one year of time.
Second, one of the unique features of Responsive Teaching is that this curriculum promotes social emotional functioning as well as cognitive and communication development. In fact, the same RT strategies that are recommended to promote pivotal behaviors related to children's cognitive and communication development are also used to promote pivotal behaviors related to social emotional development. In the evaluation of Responsive Teaching, children's progress in each of the three developmental domains had less to do with extent to which intervention focused on these domains, and more to do with how responsive children's mothers became during intervention. The instructional strategies that RT recommended to promote children's cognitive and communication development also helped to address children's social-emotional needs, even though this was not the focus of intervention.
Recently, there have been concerns regarding the number of children with Down syndrome who have either behavior problems (Cuskelly & Dadds, 1992; Coe, Matson, Russell, et al., 1999; Gath, 1986) or severe social emotional disturbances such as Autism (Capone, 2005; Howlin, 1995; Kent, 1999). One implication of these reports is that developmental interventions must not only address the cognitive and communication problems of children with Down syndrome, they must also attempt to prevent or address behavioral or social emotional problems as well. We are unaware of any developmental intervention other than Responsive Teaching that has been reported to address all three of these developmental domains. Future evaluations of Responsive Teaching with children with Down syndrome and other disabilities need to determine whether this intervention is effective at addressing the social emotional functioning of these children as well.
Third, one of the primary things that parents request from their children's early intervention program is information about what they can do at home to support or enhance their children's development. Responsive Teaching is designed specifically to address this need. Many interventionists are unsure of what they should ask parents to do at home, since often the types of activities that they do with children in classrooms or clinics do not translate easily into activities that parents can do with children during their daily routine. Because Responsive Teaching was developed from observations of how parents typically interact with their children, RT provides parents with information that can be easily incorporated into the routine activities they have with their children. When we conducted the evaluation of RT, one of the questions we were concerned about was whether RT would place additional stress on parents. We measured how stressed parents were at the beginning and end of intervention using the Parenting Stress Index (Abidin, 1995). We found that RT did not increase parents' stress, but rather was associated with slight decreases in overall stress. While parents reported that they used RT approximately 2 hours each day with their children, this occurred mostly during the normal activities they had with their children, such as feeding, bathing, dressing and other routine social and communicative exchanges.
While parents were asked to play with their children to practice RT strategies, this lasted no longer than 5 minutes at a time and only as many times during the day as parents desired. As parents became more proficient with RT strategies, intervention recommendations shifted to encouraging parents to incorporate RT strategies into their routine interactions with their children. Thus, while RT requires parents to invest small amounts of time to learn to use these strategies, the time parents are asked to devote to this intervention over and above the time they normally spend with their children decreases over time. Rather than being a burdensome intervention, most of the parents who have participated in this intervention report that RT enhances their enjoyment of being with their children.
Summary
In this paper we have described a promising new early intervention curriculum called Responsive Teaching. This curriculum is designed to help parents become more effective at promoting their children's development and social emotional well being by infusing Responsive Teaching strategies into their routine interactions with them. It evolved from research conducted with children with Down syndrome which suggested that parents promote children's cognitive and language functioning by engaging in responsive interactions with them. A one year evaluation of this curriculum showed that it was highly effective at enhancing the development of children with autism and other developmental disabilities. While only one child with Down syndrome participated in this evaluation, the research findings that led up to the development of this intervention point to the likelihood of its effectiveness with children with Down syndrome.
Correspondence
Gerald Mahoney, Ph.D • Verna Houck Motto Professor of Families and Communities, Mandel School of Applied Social Sciences, Case Western Reserve University, 10900 Euclid Avenue, Cleveland, Ohio 44106 • Tel: 216-368-1824 • E-mail: gerald.mahoney@case.edu
References
Abidin, R. (1995). Parenting Stress Index, 3 rd Edition . Odessa, FL.: Psychological Assessment Resources.
Ainsworth, M.D. & Bell, S.M. (1975). Mother-infant interaction and the development of competence. In K.J. Connelly & J. Bruner (Eds.). The Growth of Competence (pp. 97-118). New York: Academic Press.
Bagnato, S., Neisworth, J., Salvia, J. & Hunt, F. (1999). Temperament and Atypical Behavior Scale. Baltimore, MD.: Brookes.
Bailey, D.B. & Wolery, M. (1984). Teaching Infants and Preschoolers with Handicaps. Columbus, OH: Merrill.
Bates, E., Benigni, L., Bretherton, L., Camioni. L. & Volterra, V. (1979). The Emergence of Symbols: Cognition and Communication in Infancy. New York: Academic.
Bayley, N. (1969). Bayley Scales of Infant Development. New York: The Psychological Corporation.
Bowlby, J. (1969). Attachment and Loss. New York: Basic Books.
Bruner, J.S. (1975). From communication to language: A psychological perspective. Cognition, 3, 255-287.
Bruner, J. (1983). Child Talk. New York: W.W. Norton.
Bzoch, K. & League, R. (1970). The Bzoch-League Receptive-Expressive Emergent Language Scale for the Measurement of Language Skills in Infancy.
Capone, G.T. (2005). Down syndrome and comorbid autism-spectrum disorder: Characterization using the aberrant behavior checklist. American Journal Of Medical Genetics Part A, 134(4), 373-380.
Carter, A. & Briggs-Gowan, M. (2000). The Infant Toddler Social Emotional Assessment Manual. The Connecticut Early Development Project, Department of Psychology, Yale University, New Haven, CT.
Coe, D.A., Matson, J.L., Russell, D.W. et al. (1999). Behavior problems of children with Down syndrome and life events. Journal of Autism and Developmental Disorders, 29(2), 149-156.
Cuskelly, M. & Dadds, M. (1992). Behavioral problems in children with Downs syndrome and their siblings. Journal of Child Psychology and Psychiatry and Allied Disciplines, 33(4), 749-761.
Elardo, R., Bradley, R. & Caldwell, B.M. (1975). The relation of infants' home environments to mental test performances from six to thirty six months: A longitudinal analysis. Child Development, 46, 71-76.
Gath, A., (1986). Behavior problems in retarded children with special reference to Down's syndrome. British Journal of Psychiatry, 156-161.
Goleman, D. (1995). Emotional Intelligence. New York, NY: Bantam.
Guralnick, M.J. (Ed.). (1997). The Effectiveness of Early Intervention (pp. 549-576). Baltimore, MD.: Paul Brookes.
Howlin, P., (1995). The recognition of autism in children with Down syndrome - implications for intervention and some speculations about pathology. Developmental Medicine and Child Neurology, 37(6), 398-414.
Kent, L., (1999). Comorbidity of autistic spectrum disorders in children with Down syndrome. Developmental Medicine and Child Neurology, 41(3), 153-158.
Koegel, R.L., Koegel, L.K. & Carter, C.M. (1999). Pivotal teaching interactions for children with autism. School Psychology Review, 28(4), 576-594. Baltimore, MD.: Paul Brookes.
Lewis, M. & Goldberg, S. (1969). Perceptual-cognitive development in infancy: A generalized expectancy model as a function of mother-infant interaction. Merrill Palmer Quarterly, 15, 81-100.
Linder, T.W. (1993). Transdisciplinary Play-based Assessment: A functional approach to working with young children (rev. ed.). Baltimore: Paul H. Brookes Publishing Co.
Lynch, E.C. & Beare, P.L. (1990). The quality of IEP objectives and their relevance to instruction for students with mental retardation and behavioral disorders. Remedial and Special Education, 11(2), 48-55.
Mahoney, G.J. (1988a). Maternal communication style with mentally retarded children. American Journal of Mental Retardation, 93, 352-359.
Mahoney, G.J. (1988b). Communication patterns between mothers and developmentally delayed infants. First Language, 8, 157-172.
Mahoney, G. (1999). The Maternal Behavior Rating Scale-Revised. Available from the author, Mandel School of Applied Social Sciences, 11235 Bellflower Rd., Cleveland, OH 44106-7164.
Mahoney, G.J., Kim, J.M. & Lin, C.S. (in press). Parental responsiveness and children's pivotal behavior: The keys to intervention effectiveness. Infants and Young Children.
Mahoney, G.J., Finger, I. & Powell, A. (1985). The relationship between maternal behavioral style to the developmental status of mentally retarded infants. American Journal of Mental Deficiency, 90, 296-302.
Mahoney, G. & MacDonald, J. (2007) Autism and Developmental Delays in Young Children: The Responsive Teaching Curriculum for Parents and Professionals. Austin, TX: PRO-ED.
Mahoney, G. & Perales, F. (2005). A comparison of the impact of relationship-focused intervention on young children with Pervasive Developmental Disorders and other disabilities. Journal of Developmental and Behavioral Pediatrics, 26(2), 77-85.
Mahoney, G., Powell, A. & Finger, I. (1986). The maternal behavior rating scale. Topics in Early Childhood Special Education, 6, 44-56.
Mahoney, G. & Wheeden, C. (1998). Effects of teacher style on the engagement of preschool aged children with special learning needs. Journal of Developmental and Learning Disorders, 2(2), 293-315.
Piaget, J. (1963). The Psychology of Intelligence. Totowa, New Jersey: Littlefield, Adams & Co.
Pretti-Frontczak, K. & Bricker, D. (2000). Enhancing the quality of Individualized Educational Plan (IEP) goals and objectives. Journal of Early Intervention, 23(2), 92-105.
Shadish, W.R., Cook, T.D. & Campbell, D.T. (2002). Experimental and Quasi-experimental Designs for Generalized Causal Influence. New York: Houghton Mifflin.
Sparrow, S. S., Calla, D. A. & Cicchetti, D.V. (1984). Vineland Adaptive Behavior Scales. Minnesota: American guidance services.
Stern, G.G., Caldwell, B.M., Hersher, T., Lipton, E.L. & Richmond, J.B. (1969). A factor analytic study of the mother-infant dyad. Child Development, 40, 163-182.
Vygotsky, L. (1978). Mind in Society. Cambridge, MA: Harvard University Press.
Weisenfeld, R.B. (1986). The IEPs of Down syndrome children. Education and Training in Mental Retardation and Developmental Disabilities, 21(3), 211-219.

