The voice of people with Down syndrome: An EMG biofeedback study
The laryngeal muscle tension of a group of thirty people with Down syndrome was compared with that of three other groups of people: those with learning disabilities, those with functional dysphonia (that is a voice disorder caused by misuse of the vocal mechanism) and a normal control group. The scores obtained were analysed by SPSS to determine whether there were significant differences in the way in which voice is produced by the four groups. The chief finding is that the energy level needed to activate the vocal mechanism from its at rest level to its voicing level is almost twice as great for the group with Down syndrome as for the control group. Implications for therapeutic interventions are considered. It is felt that new strategies to aid voicing need to be developed. The importance of keeping up fluid levels is highlighted.
Pryce, M. (1994) The voice of people with Down syndrome: An EMG biofeedback study. Down Syndrome Research and Practice, 2(3), 106-111. doi:10.3104/reports.39
Introduction
The purpose of this study was to explore possible causes of the often acknowledged harshness, hoarseness and gruffness in the voices of people with Down syndrome (Grove and Gray 1985), Hollien and Copeland (1965), Bergendal (1976), Michael and Carney (1964) Moran (1986), Novach (1972), Paparella and Schmick (1973), Wilson (1987).
The difference could lie in the size and shape of the larynx itself. It is known that individuals with Down syndrome may have physical abnormalities such as incomplete development of the sinus areas of the skull (Benda, 1969). However, the American researchers, Weinbreg and Zlatin (1970) and Michael and Carney (1964) have run tests on the fundamental frequencies (the base note at which the larynx vibrates) in individuals with Down syndrome. They found that the frequencies were normal - or slightly above normal: the slight difference probably being accounted for by the fact that people with Down syndrome tend to be physically smaller than the general population.
Basically then, the larynxes of people with Down syndrome are producing a normal vibration. Usually the smaller the larynx, the higher the note. Women's voices are higher than men's but people with Down syndrome - although physically smaller and with average or above average fundamental frequencies - are perceived as having voices which are gruff and low pitched.
The second possibility is that the hypotonia (reduced muscle tone), which affects the muscles of individuals with Down syndrome, has an effect on the extrinsic laryngeal muscles (the strap muscles) which hold the larynx in situ and that the pharyngeal walls, which provide resonating areas above the level of the larynx, are similarly flaccid. The hypothesis here is that the gruff voice is a product of harmonics picked up by the vibrations of the muscular walls of the tract.
A third possibility is that the characteristic open mouthed posture, associated with Down syndrome, has a drying effect on the mucosal lining which extends down the oral tract and covers the laryngeal areas; changes may result from a consistently drier environment.
It is well known that for full vocal health a reasonably high intake of fluids is required (Van Lawrence, 1980).
In the researcher's experience, children with Down syndrome do not demand drinks as often as their typically developing siblings.
Questions in this research, therefore, also asked about drinking habits.
The current research focused on the second hypothesis using an electro-myographic biofeedback technique to measure the tension in the muscles surrounding the larynx.
The technique which has been used in the past to help people with functional dysphonias to modify their speaking behaviour (Andrews, Warner and Stewart 1986) is described in detail further on.
The physiology of voice
"Phonation is the production of vocal sounds resulting from the passage of currents of air through the larynx. The strength, tone, pitch and resonance of the voice area likewise dependent on the structure and neuro-muscular control of the laryngeal and respiratory systems" (Espir and Rose, 1983).
Producing voice is a complicated process depending for its success on the movements of a number of muscle groups pulling in controlled opposition to each other.
The intrinsic laryngeal musculature consists of groups of muscles which lie between the cartilagenous framework of the larynx in either side of the airway.
The extrinsic muscles hold the larynx in situ in the neck and link with the hyoid bone above and the muscles of the thorax. For a full account of the way the voice works see Luchsinger and Arnold (1965).
Methodology
The current research focussed on four groups of people (see Figure 1):
- A group of 30 individuals with Down syndrome:
16 males, 14 females - average age 29.2 years. - A group of 32 individuals with learning disabilities (but not Down syndrome):
15 males, 17 females - average age 28.6 years. - A group of 18 individuals with dysphonic problems who had been referred for voice therapy:
11 females, 8 males - average age of 45.0 years. - A group of 29 individuals to form a control group:
14 females, 15 males - average age 26.6 years.
The people with Down syndrome or learning disability were contacted through local services. The control group were volunteers.
Age range:
The lower age limit was fixed at 18 years. It was hoped to avoid any late adolescent voice changes by fixing this limit well above the general age of puberty.
The upper age limit was intended to be set to exclude changes due to diseases of ageing (the connection between Down syndrome and Alzheimer's disease has been frequently discussed). However, as many of the dysphonic group were somewhat older, it was decided to include people up to 55 years.
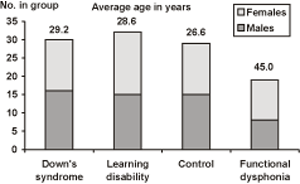
Figure 1. Composition of groups by age and sex.
People were asked to complete a questionnaire which looked at various aspects of their lives.
After general questions of fact, name, sex, age and employment etc. Question 7 asked people to rate their health - very healthy, healthy, often under the weather, poorly. Question 10 asked whether friends regarded the person as extrovert or introvert. This question had to be explained to the Down syndrome group and the learning disabilities group in terms that they could understand. Adjectives like shy, confident, outgoing, quiet, etc., were used. The decision to place a particular candidate in one or other category was then confirmed by staff or friends.
Question 11 asked people to rate their levels of perceived stress: from no stress, not very stressed, stressed or highly stressed. The EMG biofeedback is sensitive to levels of personal stress and it was important to eliminate unusual and very high levels caused by bereavement or something similar. The purpose of the question was to look at the way people viewed the level of stress in their lives. It was also appreciated that the test situation would be tense for some people although every effort was made to put subjects at their ease before applying the electrodes.
After questions relating to their history of voice problems, if any, question 15 asked people about the number of water (or water based) drinks they took during the average day. Drinks which contain caffeine, e.g. tea, coffee, coke, cola were discounted as were alcoholic drinks, because of the diuretic effect of both substances (Boone, 1983, Paparella and Shumrick 1973, Van Lawrence, 1980).
Hearing status
The high incidence of hearing loss amongst people with Down syndrome is well documented. It was felt that this additional complication should be eliminated from this voice research.
Discussions with hearing therapists established that a loss of over 20 db across the speech range in either ear could be deemed to constitute a hearing loss.
Pressures of time - and the difficulty some people with Down syndrome had in the testing situation - made it easier to settle for a sweep hearing test at 30 db across the range 250 - 4000 cycles: in both ears, using a portable Peters Audiometer. People who failed this test were, therefore, excluded from the final project.
Electromyographic biofeedback
This is a device which measures the electrical activity which occurs when a nerve impulse triggers the contraction of an individual group of fibres in a muscle.
The feedback is provided by the deflections of a needle on a dial. There is also an auditory feedback facility which gives a clicking noise into an earpiece whenever a threshold tension level is exceeded.
The auditory feedback was not used during the assessments under consideration but could have a significant role to play in the therapeutic use of the EMG Biofeedback during rehabilitation activities.
[third refernent,electrode,calibrated dial for,visual feedback,ear piece for auditory feedback on/off volume sensitivity EMG 180]
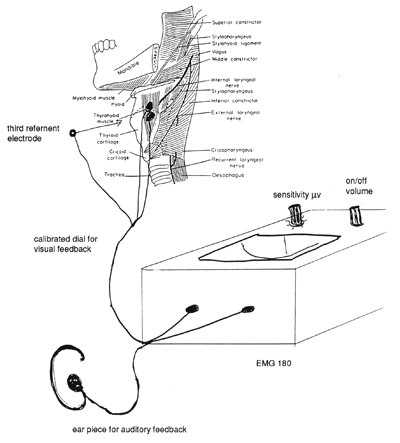
Figure 2. Diagram showing the placement of electrodes for Electromyography.
Methods of use
The recording electrodes are placed in a line along the belly of the muscle under study and a further electrode, the referent, is placed a few inches away and equidistant from the two recording electrodes (see Figure 2).
The site for the placement of the electrodes was cleaned. A pumice was used to abrade the skin in order to remove any dead cells. Electrode gel was then applied to the silver coated mesh on each of the three electrodes. The findings were cross-checked using the Vocal Profile Analysis Protocol. This is an assessment of vocal features carried out by a trained professional who analyses the position and action involved in various aspects of voicing.
Results
The three areas which brought out the most interesting results were:
- The Extroversion/ Introversion rating.
- The Hydration levels.
- The Vocal Initiation levels.
Extroversion/ Introversion Rating
The use of these terms had to be explained using words like shy, confident, outgoing, quiet etc., to groups with learning disabilities including Down syndrome. The question was asked: Do other people regard you as an extrovert or an introvert?
Obviously, ideas of esteem, self-worth and sociability were involved.
The stereotypical view of people with Down syndrome as open, easy-going, happy-go-lucky, sociable people was not borne out by the figures (see Table 1).
There is, therefore, a high level of perceived introversion amongst people with learning disabilities of all sorts.
The findings of Leudar, Frazer and Jeaves (1981), were that the posture and attitude of people with Down syndrome was more passive and less assertive than in other people.
| Group with Down syndrome | Group with learning difficulties | Control group | Group with functional dysphonia |
|---|---|---|---|
| 60% | 50% | 10% | 27.7% |
(Figures taken from the answers to the questionnaire.)
Hydration
The number of water (or water based) drinks that each person took during twenty-four hours was counted (using the questionnaire). These figures exclude drinks containing caffeine and those containing alcohol. Both caffeine and alcohol have diuretic properties.
Since many writers on "voice", including Van Lawrence (1980), Boone (1983) and Paparella and Shumrick (1973), stress the importance of keeping up appropriate fluid level for good voice health, it seemed useful to enquire into people's drinking habits. Table 2 below shows the findings.
Vocal Initiation Levels
The average person uses 72.52 microvolts of energy to initiate voice: that is to set in motion the vocal cord vibrations that are perceived as underlying so much of human communication (see Figure 3).
| Group with Down syndrome | Group with learning disability | Normal controls | Group with functional dysphonia | |
|---|---|---|---|---|
| 0-1 drink daily | 40% | 53% | 7% | 3% |
| 2-3 drinks daily | 46% | 37.5% | 7% | 16% |
| 4 or more drinks daily | 13% | 9.3% | 86% | 83% |
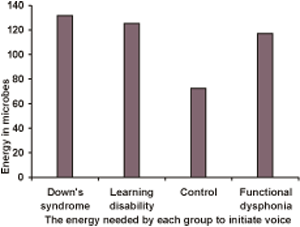
Figure 3. Energy levels measured in microvolts required to initiate voice.
The person with Down syndrome uses 131.57 microvolts to achieve the same effect (nearly twice as much).
The people with functional dysphonias who are acknowledged to have voice problems used - on average - 116.89 microvolts. For people with learning disabilities, the figure was 125.53 microvolts.
The three groups under consideration all have to expend more energy than the normal control group in achieving phonation.
The high showing of the group with learning disabilities may be explained by the number of people with cerebral palsy among their number. These findings are statistically highly significant.
The hypothesis that the hypotonia in Down syndrome gives rise to a floppy musculature, which includes a range of harmonics in the voice produced by the flaccidity of the walls of the supra-laryngeal tract, is not proven. However, greater levels of energy (effort) are needed to activate a more flaccid mechanism.
The figures for the group with Down syndrome are statistically very significant when compared with the control group. It means that whereas the average person uses 72.52 microvolts of energy to initiate voice, the individual with Down syndrome needs to use 131.57 microvolts - not far off twice as much energy to obtain the same result.
Again, the result for people with learning disabilities is high - as are all their results in these tests - but it is not as high in this case as the group with Down syndrome who are also considerably higher than the group with known voice problems.
The scores for the learning disabilities group are found to be statistically significantly different from the control group.
If initiating voice is difficult, one is less likely to put in the "back channels" which show that one is involved in the interaction. One may have something relevant to say but if it takes time to contribute comment, someone else may have seized the initiative. Your punchline may be lost. If this happens too often, you may become discouraged from ever trying to contribute.
People who cannot easily vocalise are at a disadvantage in all language learning. The telegraphic style of many young people with Down syndrome (Bray and Woolnough, 1988) may in part be due to their inability to produce voice long enough to sustain a normal length sentence.
Since language learning has important correlations with the development of cognitive processes, and oral production plays a significant part in the learning process for most speakers, it is obvious that a competent and easily useable vocal mechanism is important in general intelligibility - and, therefore, in general acceptance in the community.
Discussion
Voice therapy with people with Down syndrome
There is, as yet, little work being done to remediate the voices of people with Down syndrome. Speech and Language therapists have focussed their attention on the need to develop the language skills of children with Down syndrome who, undoubtedly, require skilled input in this area (Jenkins, 1991, Cunningham et al., 1985 etc).
The poor articulation of this group of people has also been recognised and programmes are frequently devised to assist in improving this (Hamilton, 1993). However, the current research suggests that far more emphasis needs to be placed on the problems of initiating voice. Ideally, this should be incorporated into early therapy packages so that an awareness of the problem and procedures to remediate it can be started - almost from birth.
Voice therapy techniques have traditionally developed from the strategies used by singing teachers to promote vocal control and to eliminate straining and vocal abuse. Very few people with Down syndrome can sing at all. Therapy techniques for increasing vocal efficiency need to be devised.
The EMG Biofeedback is an excellent way of enabling people to see (and hear) the tension in their own muscles. It would seem to have long term therapeutic uses as an instrument for enabling people with Down syndrome to monitor their own vocal state and, therefore, take an active part in the remediation process.
The drinking habits of people with Down syndrome have also been highlighted. Parents, schools and Training Centres could all become more aware of the need to introduce wider choices of drinks (not just coffee in the morning and tea in the afternoon). For good vocal health, can we all raise our glasses, charged with water or fruit juice, to a future which involves more drinks and lots of choices.
Acknowledgements
This research was supported by a grant from the Down Syndrome Association and an award from the College of Speech and Language Therapists. The author wishes to thank Sarah Service and Beryl Kellow, speech and language therapists, and Andrew Gammie of the Bath Institute of Medical Engineering, for their help and advice.
This research was conducted as part of a Masters Degree at the University of Portsmouth.
References
- Andrew, S., Warner, J., and Stewart, R. (1986) EMG Biofeedback and Relaxation in the Treatment of Hyperfunctional Dysphonia. British Journal of Disorders of Communication, Vol. 21. 3. 353-369.
- Beckman, D., Wold, D. and Montague, J. (1983) A Non Invasive Acoustic Method Using Frequency Pertubations and Computer Generated Vocal-tract Shapes. Journal of Speech and Hearing Research Vol. 26 304-314.
- Benda, C. (1969) Down Syndrome: Mongolism and Its Management. New York: Grune and Stratton.
- Bergendal, B. (1976) in Wilson, K. (1987) Voice Problems of Children. Williams and Wilkins.
- Boone, D.R. (1983) The Voice and Voice Therapy, 3rd Edition. Prentice Hall.
- Buckley, S.J. and Sacks, B. (1987) The Adolescent with Down Syndrome. Portsmouth Down Syndrome Trust.
- Cunningham, C.C., Glen, S.M., Wilkinson, S. and Sloper, P. (1985) Mental Ability, Symbolic Play and Receptive and Expressive Language of Young Children with Down Syndrome. Journal of Child Psychology and Psychiatry, Vol. 126 255-256.
- Espir, M. and Rose, C. (1983) The Basic Neurology of Speech and Language, 3rd Edition. Blackwell Publishers.
- Green, M. (1959) The Voice and Its Disorders, 2nd Edition. Pitman Medical.
- Greene, M. and Mathieson, L. (1989) The Voice and Its Disorders. Whurr, London.
- Groves, J. and Gray, R. (1985) A Synopsis of Otolaryngology. John Wright & Sons (Bristol).
- Hamilton, C. (1993) Investigation of the articulatory patterns of young adults with Down syndrome using electropalatography. Down Syndrome: Research and Practice, 1(1), 15-28. [Open Access Full Text]
- Hollien, H. and Copeland R. (1965) Speaking Fundamental Frequency (SFF) Characteristics of Mongoloid Girls. Journal of Speech and Hearing Disorders, 30, 344-349.
- Leuder, I., Fraser, W.I. and Jeeves, M.A. (1981) Social Familiarity and Communication in Down Syndrome. Journal of Mental Deficiency Research, 25, 133-142.
- Luchsinger, R. and Arnold, G. (1965) Voice-Speech-Language. Wadsworth Publishing Co.
- Michel, J.F. and Carney, R.J. (1964) Pitch Characteristics of Mongoloid Boys. Journal of Speech and Hearing Disorders, 121-125.
- Montague, J.C. Brown, W.S. and Hollien, H. (1974) Vocal Fundamental Frequency Characteristics of Institutionalised Mongoloids. American Journal of Mental Deficiency, 78, 414-418.
- Moran, M.J. and Gilbert, H.R. (1978) Speaking fundamental Frequency Characteristics of Institutionalised Adults with Down Syndrome. American Journal of Mental Deficiency, 83 248-252.
- Moran, M.J. and Gilbert, H.R. (1982) Selected acoustic characteristics and listener judgments of Down syndrome adults. American Journal of Mental Deficiency, 86, 553-556.
- Moran, M.J. (1986) Identification of Down syndrome adults from prolonged vowel samples. Journal of Communication Disorders, 19, 387-394.
- Moran, M., LaBarge, J. and Haynes, W. (1988) Effects of voice quality on adult perception of Down syndrome children. Folia Phoniatrica, 40, 157-161.
- Morris, A.F., Vaughan, S.E. and Vaccaro, P. (1982) Measurements of neuromuscular tone and Strength in Down Syndrome Children. Journal of Mental Deficiency Research, 26, 41-46.
- Novack, A. (1972) The voice of children with Down syndrome. Folia Phoniatrica, 24, 182-194.
- Paparella, K. and Shumrick, S. (Eds.) (1973) Otolaryngology, Vol. 3 Head and Neck. W.B. Saunders Co.
- Pentz, A.L. and Gilbert, H.R. (1983) Relation of selected acoustical parameters and perceptual ratings to voice quality of Down syndrome children. American Journal of Mental Deficiency, Vol. 88, 203-10.
- Pentz, A.L. Formant amplitude of children with Down syndrome. American Journal of Mental Deficiency, 92, 230-3.
- Pueschel, S.M. The Young Person with Down Syndrome. Transition from Adolescence to Adulthood. Paul Brookes.
- Rondal, J.A. (1988) Down Syndrome. In Bishop, D. and Mogford, K. (Eds), Language Development in Exceptional Circumstances. Churchill Livingston.
- Van Lawrence, L. (1980) Vocal Problems of the Professional User of Voice. Video from The College of Speech and Language Therapists, 7 Bath Place, Rivington Street, London, EC2A 3DR.
- Weinberg, B. and Zlatin, M. (1970) Speaking fundamental frequency characteristics of 5 & 6 year old children with mongolism. Journal of Speech and Hearing Research, 13, 418-425.
- Williamson, G (1992) Conversation Stoppers. Therapy Weekly, Vol. 19, No. 21.
- Wilson, D.K. (1987) Voice Problems of Children, 3rd ed. Williams and Wilkins.
- Woo, P. and Arandia, H. (1992) Intra-operative laryngeal electro-myographic assessment of patients with immobile vocal fold. Annals of Otology, Rhinology and Laryngology, Vol. 101, 156-158.
- Zenker, W. and Zenker, A. (1960) in Luchsinger, R. and Arnold, G. (op. cit)

