A preliminary study of intervention addressing early developing requesting behaviours in young infants with Down syndrome
Infants with Down syndrome display characteristic deficits in early communicative behaviours, including requesting. This deficit significantly and negatively impacts later communication and cognitive development. In this study, we explored intervention to address requesting in young infants with Down syndrome. Two infants with Down syndrome were taught increasingly sophisticated forms of early requesting skills (i.e., gaze shifting and gaze shifting paired with vocalisation). One of the infants was also taught a verbal approximation of the word "more". The application of interventions to address and prevent impairments characteristic of the behavioural phenotype demonstrated by infants and children with Down syndrome is discussed.
Jones, E, Feeley, K, and Blackburn, C. (2010) A preliminary study of intervention addressing early developing requesting behaviours in young infants with Down syndrome. Down Syndrome Research and Practice, 12(2), 98-102. doi:10.3104/reports.2059
Children with Down syndrome show a distinct pattern of early developing strengths and weaknesses, termed a behavioural phenotype [1] . The early deficits characteristic of this behavioural phenotype set the stage for negative outcomes in a number of areas of development (e.g., communication and cognitive development). Researchers have suggested that intervening very early in development might prevent deficits and the negative consequences associated with them [1,2] . The purpose of early intervention is to prevent the onset of deficits; therefore, intervening at a point that is "earlier" than the point at which a skill is likely to emerge in typically developing infants provides truly preventative intervention. A number of areas of communication are impaired in children with Down syndrome (e.g., delays in babbling [3] ; poor expressive language [4] ; poor articulation [5] ; delays in vocabulary and syntax [4 , 6]; problems with speech intelligibility [7] ). One of the earliest emerging communicative impairments is in requesting (e.g., refs 2, 8,9,10). Requesting involves communicative responses to regulate another person's behaviour (e.g., to access a tangible object or activity) and is first seen in typically developing infants during the latter half of the first year of life. Eye gaze (i.e., shifting gaze between an object and communicative partner), gesture use (e.g., pointing, reaching), and vocalisation are well documented early developing forms of requesting [11,12] . These forms of requesting are also those measured in assessments of early communicative behaviours (e.g., ref 13).
Requesting behaviours serve a specific function or purpose. The intent of the communication is "I want that." For example, while pointing at his bottle, an infant vocalises and looks from the bottle to his/her caregiver. Requesting involves tangible consequences, such as access to the object itself or engagement in an activity with the object [11 , 14,15,16] . The purpose of requesting contrasts with other communicative behaviours that look similar, but serve other purposes. For example, joint attention also involves gaze shifting, gesture, and vocalisation, but the function of joint attention is more social, serving to engage another person in shared attention about an object/event.
Several studies have demonstrated early emerging deficits in nonverbal requesting behaviours, but not joint attention skills, in children with Down syndrome (e.g., refs 2, 9,10). Mundy et al. found that children with Down syndrome (12 to 36 months) displayed fewer nonverbal requests, but similar joint attention skills, than their typically developing mental age matched peers [10] . Fidler et al. also found impairments in requesting skills in children with Down syndrome (average age 34.25 months) compared to typically developing children matched for mental age [8] . However, deficits were present only during requests involving objects (instrumental requests; e.g., pointing to obtain an object out of reach), not during requests that involved social interactions (e.g., looking at an adult to continue a song), a finding also reported by Mundy et al. [2] .
Early requesting behaviours are particularly important as they are related to later communicative and cognitive competence. This has been demonstrated for both typically developing children and those with disabilities of other aetiologies (e.g., autism) (e.g., ref 17) as well as children with Down syndrome [2] . In children with Down syndrome, early requesting behaviours are correlated with language development [2 , 8, 10] as well as problem solving skills [8] . Communication impairments also increase the likelihood of challenging behaviour [18] . In children with Down syndrome, early deficits in fundamental communication skills such as requesting may exacerbate an already existing propensity to engage in challenging behaviour [19,20] .
In a recent review of language and communication development in individuals with Down syndrome, Roberts, Price, and Malkin noted that, despite the significant communication impairments in individuals with Down syndrome, "relatively little research has focused on the effectiveness of intervention strategies for improving the communication skills of individuals with Down syndrome"[ 21:p.30] . This is certainly true of early requesting skills; only a handful of studies exist examining interventions to teach requesting skills an specifically to very young children with Down syndrome. The existing intervention research has involved participants of varying diagnoses, with only some of the participants having a diagnosis of Down syndrome. Prelinguistic milieu teaching (PMT) is one intervention that has been examined to specifically teach requesting skills and, in a handful of studies, some participants had Down syndrome. PMT involves arranging the environment (e.g., high interest activities are available) and following the child's attentional lead (e.g., interventionist engages in child selected activities), as well as engaging in social routines (e.g., turn taking games) [22] .
Mand model refers to a teaching procedure in which the interventionist mands (instructs) a learner to engage in a specific communicative response (e.g., the interventionist says, "Tell me what you want."). If the learner produces an incorrect response, the interventionist then models (e.g., the interventionist says, "Say, 'I want juice.'") the desired communicative response. Correct responses (following a mand and/or a model) result in praise. See Halle [42] and Rogers-Warren & Warren [43] for additional information.
Correct responses are prompted using specific questions, models, and directives to imitate (i.e., mand model) and result in naturally occurring consequences (i.e., access to the object requested). For example, during a one on one session, the interventionist engages the child in a play activity and then stops on his/her turn creating a situation in which the child should request continuation. Specific prompts (e.g., "Look at me") are used. Target responses result in reinforcement involving continuation of the activity and specific praise ("You looked at me!"). Unfortunately, much of the research on PMT has not reported results specifically for the children with Down syndrome [22,23] .
In two early studies, Warren, Yoder, Gazdag, Kim, and Jones and Yoder, Warren, Kim, and Gazdag demonstrated the effectiveness of prelinguistic milieu teaching to specifically address requesting skills (e.g., gaze shift from an object to interventionist in conjunction with a reach to the object) in children with developmental disabilities [24,25] . Of the 9 participants across both investigations, 4 children had Down syndrome (20-26 months). Interestingly, in two recent studies, a larger subgroup of the participants had Down syndrome (43 of the 90 total participants across both studies), allowing for an examination of the effects of intervention specifically for children with Down syndrome (mean age 22-26 months across the intervention and control groups in both studies) [26,27] . Intervention involved prelinguistic milieu teaching in conjunction with responsive education (RE) which focused on improving parents' awareness of their child's communication acts and provision of appropriate responses to these acts. However, the findings from the two studies are conflicting. Yoder and Warren concluded that, with respect to the development of early requesting skills, RE and PMT "appeared to decelerate growth in requests in children with Down syndrome" [26: p.1169] . They suggested this may have been due to the motor demands of the gestures that may be more difficult for children with Down syndrome to produce (the target forms of requesting involved gaze shifting combined with either gestures [such as pointing or reaching] or vocalisations). In contrast, Fey et al. found increases in communication by the group who received RE/PMT compared to a no treatment control group, with no differences for the subgroup of participants with Down syndrome [27] . The differences in results across these studies for children with Down syndrome may be due to the way that Fey et al. implemented intervention. Fey et al. initially targeted less complex forms of requesting (e.g., only a gaze shift) and then increased the expectations (e.g., to a combination of gaze shifting and vocalisation or gesture) as children acquired requesting skills.
Present study
The deficits in requesting and relation of early requesting to language and cognitive development as well as challenging behaviour, in addition to a preventative focus of intervention, suggest the need to further examine intervention to address this area of deficit in young infants with Down syndrome. With the early identification of Down syndrome, intervention can begin shortly after birth. It is possible to examine the application of intensive intervention procedures to teach requesting behaviours to infants with Down syndrome (less than 1 year of age), at the age when typically developing children begin demonstrating requesting [11 , 13] . Similar to the work of Fey et al. [27] and given the focus of this study being on young infants, intervention procedures were introduced to establish increasingly sophisticated forms of requesting. In this preliminary study, we explored the application of intervention procedures to establish early requesting behaviours that combine gaze shifting and vocalisations as well as increasingly specific vocalisations (e.g., word approximation) in young infants with Down syndrome.
Method
Participants
The parent(s) of two infants with Down syndrome provided informed consent for participation in this study. Josh was 6 months old. He was the only child in his family and his mother was his primary caregiver. Josh's performance on the Preschool Language Scale - Third edition [28] , conducted when he was 5 months of age, indicated an age equivalent of 0-5 months for auditory comprehension and 0-4 months for expressive communication. Josh performed within normal limits on the Rossetti Infant Toddler Language Scale-Second Edition [29] . On the Receptive-Expressive Emergent Language Scale - II [30] , Josh's receptive language was at the 4-5 month level, however, expressively, he performed at the 2-3 month level. At 1 month of age, Josh was enrolled in a home based intervention programme that utilised a transdisciplinary approach in which professionals, acting as primary interventionists, conducted the interventions designed and overseen by related service personnel representing several developmental areas. For Josh, a special educator and a physical therapist conducted 90 minute intervention sessions, three times per week, addressing physical, speech/language, and cognitive goals as well as parent training. Josh was described by his family and interventionists as a very social baby (i.e., he smiled often). He vocalised to gain his parents' attention, engaged in reciprocal babbling, and was beginning to understand cause and effect relationships. Josh's intervention goals included increasing head control, holding toys, responding to his name, and increasing vocalisations.
Betty was 9 months old. Her mother was her primary caregiver. At the time of the study, the most recent assessment information available had been conducted when Betty was 4.5 weeks of age. The Hawaii Early Learning Profile [31] and the Preschool Evaluation Scale [32] indicated Betty was performing within normal limits across developmental domains (i.e., communication, cognitive, social emotional, adaptive behaviour, and motor skills). However, according to the Peabody Developmental Motor Scales - Second Edition [33] , Betty's motor skills were found to be delayed (31st percentile). From the age of 1.5 months, Betty had been receiving early intervention services consisting of two 45 minute physical therapy sessions per week and two 60 minute parent training sessions conducted by a special educator. Betty was described by her interventionists and mother as a very social child. She responded to her name, vocalised to gain adult attention, and was proficient in activating age appropriate cause and effect toys. Betty's interventionists and mother were addressing motor skills such as getting in and out of a seated position and crawling, play skills, and communication skills such as lifting her arms to be picked up as well as waving hello and goodbye.
Setting and interventionists
All baseline and intervention procedures were implemented in the infants' homes. Josh's intervention was implemented in his nursery and Betty's intervention was implemented in her living room. Josh's special educator (second author) and Betty's mother (both referred to as interventionists throughout the rest of this study) implemented all intervention procedures.
Requesting activities
Each child's parents were asked to identify toys they felt were particularly interesting to their child. To prevent satiation (e.g., infant failing to look at the activated toy), at least five different toys were used over the course of intervention for each infant. Josh's toys consisted of two different colourful rattles, two small colourful stuffed animals (one that also vibrated), and a plush cartoon character. Betty's toys consisted of two different colourful rattles, two different small stuffed animals, and a small doll.
Response definitions
The forms of requesting taught in this study were similar to those observed in assessments of early communication (including requesting) [13] and taught in other requesting intervention studies (e.g., ref 27).
Gaze shift
A gaze shift consisted of the infant looking from the preferred object to his/her interventionist within 10 seconds of the interventionist's discontinuation of action with the object.
Prompted vocalisation
A prompted vocalisation consisted of the infant emitting a vocalisation (i.e., open mouth sound) following the interventionist gently tapping the infant's lips with the tips of her fingers.
Gaze shift and vocalisation
Gaze shift and vocalisation consisted of the infant independently looking from the preferred object to his/her interventionist while at the same time independently (i.e., without prompts) vocalising, within 10 seconds of the discontinuation of action with the object.
Gaze shift and verbal approximation of a requesting response
Gaze shift and verbal approximation consisted of the infant shifting looking from the preferred object to his interventionist while at the same time emitting an approximation of the word "more," specifically "mmm," within 10 seconds of the discontinuation of action with the preferred object. This response was only taught to Josh. Due to scheduling conflicts, Betty was unable to continue participating in this study after she acquired the gaze shift and vocalisation requesting response.
Design
An AB design within which intervention was sequentially introduced to address increasingly sophisticated forms of the requesting response was used. That is, the first target behaviour (i.e., gaze shifting) was addressed via intervention and, once the infant acquired that response, intervention was applied to teach a more sophisticated form of requesting (i.e., gaze shift and vocalisation). For Josh, intervention was sequentially applied to three increasingly sophisticated requesting responses (i.e., gaze shift; gaze shift and vocalisation; and gaze shift and verbal approximation of a requesting response). Betty's participation in this study ended early due to scheduling conflicts; therefore, intervention was sequentially applied to only two increasingly sophisticated requesting responses (i.e., gaze shift followed by gaze shift and vocalisation).
Procedure
All procedures (during baseline and intervention) were conducted while the infant and interventionist were engaged in toy play with one of the preferred toys that parents had identified previously. Each infant sat in an infant seat while the interventionist sat directly in front of him/her.
Baseline
During each baseline opportunity, the interventionist engaged the child in play with one of the preferred toys (e.g., rattle, stuffed animal), activating the toy by shaking it and moving it closer to the infant and then pulling it out of his/her reach, but keeping it in the infant's visual field. After repeating this motion three to five times (depending on how quickly the interventionist could gain the infant's attention on the toy), the interventionist stopped the toy, moved it out of the infant's reach, and waited 10 seconds for the infant to shift his/her gaze from the object to the interventionist, either in isolation or paired with a vocalisation or verbal approximation. During baseline, no feedback was given to the infant. That is, the opportunity was terminated (i.e., the toy was removed) regardless of infant response (e.g., either upon gaze shifting [in isolation or paired with a vocalisation or verbal approximation] or no response) at the end of the 10 second interval. Each baseline session consisted of five opportunities. For Josh, three baseline sessions were conducted on 2 different days. For Betty, two baseline sessions were conducted on 2 different days. Both infants clearly demonstrated the absence of responding, therefore, additional baseline opportunities did not seem warranted.
Intervention
Intervention opportunities began the same way as baseline opportunities. That is, the interventionist engaged the child in play with one of the preferred toys (e.g., rattle, stuffed animal), shaking it and moving it closer to the infant and then pulling it out of his/her reach. After repeating this motion three to five times, the interventionist stopped the toy and moved it out of the infant's reach. Once the infant correctly requested that the interventionist continue activity with the toy (either independently or following a prompt, discussed next), the interventionist provided praise, social interaction, and reactivated the toy.
Gaze shift
Prompting of gaze shifting involved the interventionist moving her face into the infant's line of vision and/or making a noise (e.g., taking in a deep breath, clicking her tongue). For Josh, during the initial intervention sessions, the interventionist immediately (0 second time delay) prompted him to engage in the target response. That is, as soon as the interventionist pulled the toy out of Josh's reach, she prompted him to shift his gaze. Prompts were faded by inserting a 10 second delay prior to delivering the prompt (i.e., a time delay procedure) and then faded from a full prompt (i.e., the interventionist moving her face into Josh's line of sight while making a noise consisting of several tongue clicks or taking a deep breath) to a partial prompt (i.e., only making tongue clicks or taking a deep breath), and finally to a minimal prompt (i.e., one tongue click emitted at a very low volume or a quick breath) (i.e., a most to least prompt fading procedure).
Betty's team preferred not to implement prompts immediately and, therefore, intervention began with a 10 second delay during which Betty could respond. If Betty did not engage in gaze shifting by the end of the 10 second interval, the response was prompted using the same form of prompting used for Josh (i.e., moving into the infant's line of vision and making a noise). Prompts were also faded using a most to least prompt hierarchy. That is, once Betty consistently responded to the full prompt (i.e., the interventionist moving her face into Betty's line of sight while making a noise consisting of several tongue clicks or taking a deep breath), a partial prompt was used (i.e., making several tongue clicks or taking a deep breath), and finally a minimal prompt (i.e., one tongue click emitted at a very low volume or a quick breath).
For both infants, once they engaged in gaze shifting (either independently or following a prompt), the interventionist reactivated the toy (i.e., shook the stuffed animal closer to the infant) and smiled, in conjunction with verbal praise (e.g., "That was good looking!") and physical interaction (e.g., a tickle, hug, or rubbing his/her arms, legs, or belly). That is, the interventionist delivered reinforcing consequences including the natural consequences for requesting (in this case, reactivating the toy) following the infant's requesting response. Mastery criterion was 80% or more independent responding across two sessions and 2 days.
Establishing a promptable vocal response
To ensure the infant would tolerate physical prompts to the facial area, specifically the lips, so that vocal responses could be prompted, parents were instructed to manipulate the child's mouth area several times per day. Specifically, during everyday activities such as diaper changes, playtime, and mealtime, parents gently tapped, stroked, and pressed their infant's lips.
A prompted vocal response was the emission of a vocalisation (i.e., open mouth sound) when the caregiver gently tapped the infant's mouth with the tips of his/her fingers. Parents initially tapped the infant's mouth while the infant vocalised throughout the day. For example, if the infant began to vocalise while sitting in his highchair, his parent would approach and gently tap on the infant's lips. When the infant continued to vocalise, his parents delivered social reinforcement (e.g., verbal praise ["Way to go!"], tickles, and/or picking up the infant and holding him). Over time, both Josh and Betty's parents were able to gently tap their infant's lips and he/she would consistently respond by vocalising, thus, establishing a promptable vocal response.
Gaze shift and vocalisation
As each infant met mastery criterion (80% or more independent responding across two sessions and 2 days) for gaze shifting, the criterion for correct responding changed to a more sophisticated requesting response (i.e., the infant was not only required to shift his/her gaze from the toy to the interventionist, but also to vocalise). Intervention began in the same way as when gaze shifting alone was taught. While playing with one of the toys, the interventionist shook the toy, moving it closer to and farther away from the infant, eventually pulling the toy out of the infant's reach. As the infant had already acquired gaze shifting, he/she looked at the interventionist waiting for the toy to be reactivated. For Josh, once he shifted his gaze, the interventionist immediately prompted him to make an open mouth vocalisation (i.e., tapping his lips with her fingers). Prompts were faded by inserting a 10 second delay prior to delivering the prompt (i.e., time delay procedure) and then changing the full prompt (i.e., tapping Josh's lips) to a less intrusive prompt (i.e., putting her index and middle fingers up towards Josh's lips), and then finally to a minimal prompt (i.e., the interventionist just raised her two fingers) (i.e., a most to least prompt fading procedure).
As had been done to teach gaze shifting to Betty, her intervention began using a 10 second delay. If Betty did not respond within 10 seconds, she was prompted to do so. The same prompt was used with Betty as with Josh, along with a most to least prompt fading procedure. (Although a rare occurrence, if either infant did not engage in the previously taught behaviour [i.e., gaze shift], he/she was prompted to emit that target behaviour and then prompted to emit the more sophisticated response.)
For both infants, after they shifted their gaze and vocalised, the interventionist delivered reinforcement (i.e., reactivated the toy and smiled in conjunction with verbal praise and physical interaction). Mastery criterion was 80% or more independent responding across two sessions and 2 days.
Gaze shift and verbal approximation of a requesting response
Due to scheduling conflicts, Betty's involvement in the study ended after teaching her to shift her gaze and vocalise. Therefore, this final intervention condition was implemented only with Josh. Once Josh met criterion for mastery (i.e., 80% or more independent responding across two sessions and 2 days) of gaze shifting with vocalisation, the criterion for correct responding changed to include shifting his gaze and verbalising an approximation (i.e., "mmm") of a requesting response (the word "more"). Josh's educational team members considered verbal approximations as appropriate intervention targets because Josh was just beginning to use the word "dada" when he saw his father. In addition, "mmm" was a verbal approximation that he could easily use across activities and environments (e.g., during meal time, playing with toys, singing with his family).
Once the interventionist engaged Josh with the preferred toy, moving it closer to and farther away from him and eventually pulling it out of his reach, Josh shifted his gaze and vocalised as he had been taught previously. At this point, both a physical prompt and a model of the target verbalisation were used to prompt the more sophisticated verbal response (i.e., "mmm"). That is, while Josh vocalised (an open mouth vocalisation), his interventionist gently applied pressure to his upper and lower lips so that his lips closed, and the sound became, "mmm" (an approximation for "more"). Simultaneously, the interventionist modelled the "mmm" sound. Prompts were delivered immediately (i.e., 0 second time delay) and faded using a time delay (i.e., inserting a 10 second delay before delivering the prompt) paired with a most to least prompt hierarchy (from a full prompt to a partial prompt in which the interventionist provided the verbal model, but only raised her hand up to Josh's mouth, without touching him) as had been done previously during intervention. (If Josh did not engage in the previously taught behaviours [i.e., gaze shift with vocalisation], he was prompted to emit these target behaviour(s) and then prompted to emit the word approximation.) As soon as Josh shifted his gaze and emitted the "mmm" sound, the interventionist delivered consequences consisting of reactivating the toy and smiling in conjunction with verbal praise and physical interaction. Mastery criterion was 80% or more independent responding across two sessions and 2 days.
Reliability
Response reliability data were collected by the second author for 46% of opportunities for Betty, distributed across each condition (i.e., baseline and intervention). The number of agreements was divided by the total number of agreements plus disagreements and multiplied by 100 to obtain the percentage of agreement. An agreement was noted if the second author and interventionist (i.e., mother) scored the opportunity in the same way (as correct or incorrect). Percent agreement for response reliability cumulated across all opportunities was 96%. Unfortunately, reliability data were not collected for Josh.
Fidelity of implementation
To ensure intervention was conducted as designed, for the same 46% of opportunities for which reliability data were collected for Betty, the second author also recorded fidelity of implementation data. That is, each intervention opportunity was examined for the accurate presentation of each component of intervention (i.e., presentation of requesting opportunities, prompting procedure, and provision of appropriate consequences). The number of times the interventionist (i.e., mother) correctly presented the instructional component was divided by the total number of correct plus incorrect presentations of that component, multiplied by 100, to obtain the percentage of correctly implemented intervention procedures. Agreement was 100% for the correct presentation of requesting opportunities, 94% for the correct prompting procedures, and 100% for delivery of reinforcement.
Results
Figures 1 and 2 illustrate Josh's and Betty's independent performance, respectively. During baseline, Josh did not demonstrate gaze shifting (Figure 1), nor did he show gaze shifting paired with vocalisation or verbal approximation. The interventionist immediately prompted (i.e., 0 second time delay) eye gaze for six sessions (indicated by a session break in Figure 1). As the prompts were faded, Josh met criterion for mastery of gaze shifting within 14 sessions. When the criterion response was changed to include a vocalisation, the interventionist immediately prompted (i.e., 0 second time delay) gaze shifting and vocalisation for three sessions (indicated by a session break in Figure 1). Within nine sessions, Josh mastered gaze shifting and vocalisation. Following this phase, the criterion response was changed to include a verbal approximation (i.e., "mmm"). The interventionist immediately prompted (i.e., 0 second time delay) a gaze shift and verbal approximation for three sessions (indicated by a session break in Figure 1), after which Josh mastered this final skill within just three additional intervention sessions.
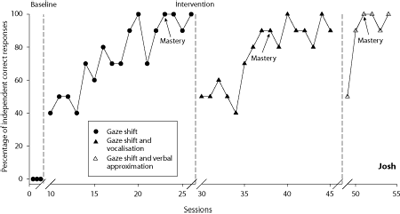
Figure 1 | Percentage of independent correct responses per session for Josh during baseline and intervention for gaze shift, gaze shift and vocalisation, and gaze shift and verbal approximation of a requesting response
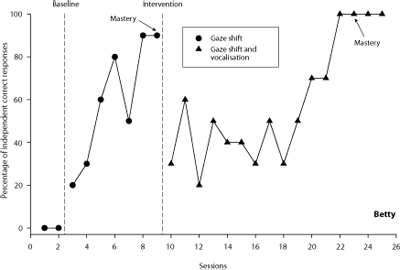
Figure 2 | Percentage of independent correct responses per session for Betty during baseline and intervention for gaze shift and then gaze shift and vocalisation
As shown in Figure 2, during baseline, Betty did not demonstrate gaze shifting nor gaze shifting paired with vocalisation. Recall that Betty's interventionist began intervention with a 10 second delay (i.e., there was no 0 second time delay); hence, Figure 2 does not depict any session breaks. Within seven sessions of intervention, Betty met criterion for gaze shifting. When the criterion was changed, she mastered gaze shifting with vocalisation within another 14 sessions. Recall that Betty was only taught gaze shifting and gaze shifting paired with a vocalisation (her participation in the study was terminated early due to scheduling conflicts).
Discussion
This study demonstrated that intervention can be used to establish increasingly sophisticated combinations of requesting behaviours, specifically the use of gaze shifting paired with vocalisation, in young infants with Down syndrome. The emergence of requesting skills in infancy marks an important shift in development from dyadic interactions between infant and caregiver to triadic interactions involving infant, caregiver, and objects in the environment. Developmental psychologists suggest this shift marks critical changes in the ability to coordinate attention amongst self, other, and object as well as intentionality and representational ability [11 , 34] . Certainly better requesting skills are associated with facility in other areas of development [2 , 8, 10] , making requesting skills important foundational skills upon which to build more sophisticated communication as well as cognitive abilities. In addition, deficits in communication skills such as requesting may exacerbate the already existing propensity for challenging behaviour that also marks the behavioural phenotype of Down syndrome [19,20] .
Although this was a case study with only 2 infants and warrants replication, the results draw attention to the application of intervention strategies to address specific communication deficits before they become pronounced areas of impairment. The young infants in this study were at the age when the earliest of requesting skills are just beginning to be demonstrated by typically developing infants. Thus, intervention was applied in a preventative manner rather than waiting to see if deficits emerged in the participants (a likely outcome given research indicating such deficits in children with Down syndrome). Intervening prior to the emergence of the deficit may not only result in the amelioration of the development of such deficits in early requesting, but also in the prevention of the negative outcomes resulting from impairments. It will be important for future research to follow infants (who have received intervention addressing requesting deficits) longitudinally to examine this question.
In this study we focused on increasingly sophisticated forms of requesting involving gaze shifting and vocalisation. For one child, three forms (i.e., gaze shifting, gaze shifting paired with vocalisation, and gaze shifting paired with a verbal approximation) of requesting were systematically addressed and, for the second child (due to schedule conflicts resulting in her early termination from the study), two forms (i.e., gaze shifting and gaze shifting paired with vocalisation). Requesting intervention addressing gestures, such as pointing, may also be particularly useful for infants and children with Down syndrome, as gestures provide an additional means of clearly expressing oneself. Gestures may be helpful in situations in which the desired object and/or the infant's communicative partner are at a distance or the desired object is one in an array of several (e.g., multiple toys on a shelf). Gestures can be taught through modelling or physical assistance and have been taught to young children as part of requesting skills (e.g., refs 24,25, 27, 35) and as part of skills serving other communicative functions (e.g., ref 36) such as joint attention [37] . The effectiveness of intervention procedures to teach gestures to young infants with Down syndrome remains to be demonstrated.
With respect to teaching gestures, Yoder and Warren suggested that their negative findings with respect to requesting skills in children with Down syndrome following intervention may have been related to the motor demands of the gestural components of the response taught [26] . However, motor issues (i.e., hypotonicity) common in children with Down syndrome have been discounted as an explanation for the lack of requesting [10] . Despite deficits in requesting, children with Down syndrome use similar forms (including gesture) to engage in joint attention interactions. Alternatively, the multicomponent nature of the response (e.g., gaze shift paired with gesture) may prove more difficult to teach (and/or to acquire). When teaching multicomponent responses, the sequential introduction of intervention to increasingly more difficult forms, as done in this study, may be important in facilitating acquisition. We have found this when teaching multicomponent communicative responses for different functions (i.e., joint attention) to children with autism [37,38] . Fey et al. initially accepted simpler forms of requesting followed by requiring combinations of gaze shifting and vocalisations or gestures resulting in positive results [27] . Similarly, in the present study, the multicomponent response of gaze shifting and vocalisation was taught sequentially, first teaching gaze shifting and then requiring the combination of gaze shifting and vocalisation. Sequentially introducing intervention may also be particularly important when adding additional components, such as gesture to a request consisting of gaze shift and vocalisation.
Requesting is, by definition, the use of specific forms serving a specific function (i.e., to obtain objects or assistance from another person). It is apparent this was the purpose of the communicative behaviours taught to these young infants. The requesting forms and situations are the same types as those in other intervention [24,25 , 27] and assessment [13] research, suggesting they reflect requesting and not another communicative function (e.g., joint attention). In addition, once the infant engaged in the communicative response and the interventionist reactivated the toy, the infant's communicative response stopped. That is, following reactivation of the toy, the infant did not continue emitting the same or other communicative responses, suggesting the infant had, in fact, obtained what he/she desired (i.e., toy reactivation). Finally, across opportunities, the provision of consequences involving reactivation of the toy resulted in an increase in the target response (i.e., the response was reinforced). Thus, reactivation of the toy which functioned as a reinforcer, substantiated the purpose of the target response was a request.
As in other intervention research on requesting in toddlers with Down syndrome (e.g., refs 24,25, 27), in this study, requests involved continued interaction with a preferred toy. This is an age appropriate type of request for young infants as they engage in simple interactive toy play with their caregivers. Fidler et al. described other types of requesting situations such as requests for social interactions that do not involve objects (e.g., the child requests a caregiver continue singing) and more instrumental requests (e.g., the child requests help obtaining a desired item) [8] . With respect to these different types of requests, Fidler et al. found that children with Down syndrome show more significant deficits in instrumental than social requests [8] . The requesting situation in this study appears to fit between these two such that the presence of the toy prevents it from being purely social, however, the activity being requested involved interaction with an adult, preventing it from being purely object focused. Importantly, intervention resulted in the acquisition of requesting skills reflective of a bridge between these two types of requesting. Differences in performance of children with Down syndrome across different types of requesting situations highlights the need to ensure that, when taught requesting skills, the infant generalises those skills across situations including those that reflect different types of requests as well as different partners. This should be examined in future research.
Requesting skills are particularly important as they are related to other areas of development, including cognition, communication, and challenging behaviour. Teaching requesting skills may provide a foundation for development in other areas. The idea that teaching one skill will lead to positive changes in related areas is consistent with the concept of pivotal skills from the behaviour analytic literature [39] . In this case, learning by 12 months of age to successfully recruit a caregiver to continue an activity with a desired toy, may result not only in procurement of the activity, but an immediate increase in the number and length of interactions between the child and their caregiver and improvement in quality of interactions, both of which may further result in improvements in development. In fact, Yoder et al. demonstrated that, after children were taught requesting skills, parents and teachers increased their interactions with the children, specifically, their use of linguistic mapping (i.e., verbalising what the child was communicating nonverbally) [25] . Further research is necessary to explore the collateral improvements associated with intervention addressing early requesting skills including language and cognitive skills, challenging behaviour, and even quality of caregiver-infant interactions.
As this was a case study with only 2 infants, replication is clearly warranted, but the effectiveness of intervention procedures to specifically address core deficits that characterise the behavioural phenotype of Down syndrome suggests, as others [8] have, that it is possible to specifically address these areas of weakness and to do so in a preventative manner, before such deficits become pronounced. Important avenues for future research include the examination of intervention applied to a variety of types of requests as well as additional forms (e.g., gesture) of requesting in young infants with Down syndrome. Future research should also involve evaluation of improvements in related areas of development when early developing skills are successfully addressed. The effectiveness of this intervention further suggests the need to continue to explore applications of preventative intervention procedures to address other core characteristics of the behavioural phenotype of Down syndrome (e.g., challenging behaviour [20] ; spontaneous communication [40] ; literacy skills [41] ).
References
- Fidler DJ. The emerging Down syndrome behavioral phenotype in early childhood: Implications for practice. Infants and Young Children. 2005;18:86-103.
- Mundy P, Sigman M, Kasari C, Yirmiya N. Nonverbal communication skills in Down syndrome children. Child Development. 1988;59:235-249.
- Lynch MP, Oller DK, Steffens ML, Levine SL, Basinger DL, Umbel VM. Onset of speech-like vocalizations in infants with Down syndrome. American Journal on Mental Retardation. 1995;100:68-86.
- Miller JF. Profiles of language development in children with Down syndrome In: Miller JF, Leddy M, Leavitt LA, editors. Improving the communication of people with Down syndrome. Baltimore: Paul H. Brookes; 1999. p.11-39
- Miller J, Leddy M, Miolo G, Sedey A. (1995). The development of early language skills in children with Down syndrome. In: Nadel L, Rosenthal D, editors. Down syndrome: living and learning in the community. New York: Wiley-Liss; 1995. p. 115-120.
- Chapman R, Hesketh L, Kistler D. Predicting longitudinal change in language production and comprehension in individuals with Down syndrome: Hierarchical linear modeling. Journal of Speech, Language, and Hearing Research. 2002;45:902-915.
- Kumin L. Intelligibility of speech in children with Down syndrome in natural settings: Parents' perspectives. Perceptual Motor Skills. 1994;78:307-314.
- Fidler DJ, Philofsky A, Hepburn SL, Rogers SJ. Nonverbal requesting and problem solving by toddlers with Down syndrome. American Journal on Mental Retardation. 2005;4:312-322.
- Jones, O. Mother child communication with prelinguistic Down's syndrome and normal infants. In: Schaffer R, editor. Studies of mother-infant interaction. New York: Academic Press; 1977. p.205-225.
- Mundy P, Kasari C, Sigman M, Ruskin E. Nonverbal communication and early language acquisition in children with Down syndrome and in typically developing children. Journal of Speech and Hearing Research. 1995;38:157-167.
- Bates E, Benigni L, Bretherton I, Camaioni L, Volterra V. The emergence of symbols: cognition and communication in infancy. New York: Academic Press; 1979.
- Bruner J. The social context of language acquisition. Language and Communication. 1981;1:155-178.
- Mundy P, Delgado C, Block J, Venezia M, Hogan A, Seibert, J. A manual for the abridged Early Social Communication Scales. 2003 [cited June 12, 2008]. Available from https://www.psy.miami.edu/faculty/pmundy/ESCS.pdf
- Bates E, Camaioni L, Volterra V. The acquisition of performatives prior to speech. Merrill-Palmer Quarterly. 1975;21:205-226.
- Bruner J, Sherwood V. Thought, language, and interaction in infancy. In: Call JD, Galenson E, Tyson RL, editors. Frontiers of infant psychiatry. New York: Basic Books; 1983. p.38-55.
- Mundy P. Joint attention and social-emotional approach in children with autism. Development and Psychopathology. 1995;7:63-82.
- Moore C, Dunham P, editors. Joint attention: its origins and role in development. Hillsdale, NJ: Erlbaum; 1995.
- Carr EG, Levin L, McConnachie G, Carlson JI, Kemp DC, Smith CE. Communication-based intervention for problem behavior: a user's guide to producing positive change. Baltimore, MD: Paul H. Brookes; 1994.
- Feeley KM, Jones EA. Addressing challenging behavior in children with Down syndrome: The use of applied behavior analysis for assessment and intervention. Down Syndrome Research and Practice. 2006;11:64-77. [Open Access Full Text]
- Feeley KM, Jones EA. Strategies to address challenging behavior in children with Down syndrome. Down Syndrome Research and Practice, [cited August 3, 2007]. [Open Access Full Text]
- Roberts JE, Price J, Malkin, C. Language and communication development in Down syndrome. Mental Retardation and Developmental Disabilities Research Reviews. 2007;13:26-35.
- Yoder PJ, Warren SF. Maternal responsivity predicts the prelinguistic communication intervention that facilitates generalized intentional communication. Journal of Speech, Language, and Hearing Research. 1998;41:1207-1219.
- Yoder PJ, Warren SF. Relative treatment effects of two prelinguistic communication interventions on language development in toddlers with developmental delays vary by maternal characteristics. Journal of Speech, Language, and Hearing Research. 2001;44:224-237.
- Warren SF, Yoder PJ, Gazdag GE, Kim K, Jones HA. Facilitating prelinguistic communication skills in young children with developmental delay. Journal of Speech and Hearing Research. 1993;36:83-797.
- Yoder PJ, Warren SF, Kim K, Gazdag G. Facilitating prelinguistic communication skills in young children with developmental delays II: Systematic replication and extension. Journal of Speech and Hearing Research. 1994;37:841-851.
- Yoder PJ, Warren SF. Effects of prelinguistic milieu teaching and parent responsivity education on dyads involving children with intellectual disabilities. Journal of Speech, Language, and Hearing Research. 2002;45:1158-1174.
- Fey ME, Warren SF, Brady N, Finestack LH, Bredin-Oja SL, Fairchild M, Sokol S, Yoder PJ. Early effects of responsivity education/ prelinguistic milieu teaching for children with developmental delays and their parents. Journal of Speech, Language, and Hearing Research. 2006;49:526-547.
- Zimmerman IL, Steiner VG, Pond RE. Preschool Language Scale (PLS-3) (3rd ed.). San Antonio, TX: The Psychological Corporation; 1992.
- Rossetti L. Rossetti Infant Toddler Language Scale (2nd ed.). East Moline, IL: Linguisystems; 1986.
- Bzoch KR, League R. Receptive Expressive Emergent Language Scale (REEL) (2nd ed.). Austin, TX: Pro-ed; 1991.
- Furano S, O'Reilly K, Hosaka C, Inatsuka T. Hawaii Early Learning Profile (HELP): Checklist (0-3). Palo Alto, CA: VORT Corporation; 1994.
- McCarney SB, Anderson PD. Preschool Evaluation Scale. Columbia, MO: Hawthorne Educational Services; 1992.
- Folio MR, Fewell RR. Peabody Developmental Motor Scales (PDMS-2) (2nd ed.). Itasca, IL: Riverside; 2000.
- Bretherton I. Intentional communication and the development of an understanding of mind. In: Frye D, Moore C, editors. Children's theories of mind: mental states and social understanding. Hillsdale, NJ: Lawrence Erlbaum; 1991. p. 49-75.
- Carr EG, Kemp DC. Functional equivalence of autistic leading and communicative pointing: Analysis and treatment. Journal of Autism and Developmental Disorders. 1989;19:561-578.
- Buffington DM, Krantz PJ, McClannahan LE, Poulson CL. (1998). Procedures for teaching appropriate gestural communication skills to children with autism. Journal of Autism and Developmental Disorders. 1998;28:535-545.
- Jones EA, Carr EG, Feeley KM. Multiple effects of joint attention intervention for children with autism. Behavior Modification. 2006;30:782-834.
- Jones EA, Feeley KM. Parent implemented joint attention intervention for preschoolers with autism. Journal of Speech-Language Pathology and Applied Behavior Analysis. 2007;2:252-268.
- Koegel LK, Koegel RL, Harrower JK, Carter CM. Pivotal response intervention I: Overview of approach. Journal of the Association for Persons with Severe Handicaps. 1999;24:174-185.
- Feeley KM, Jones EA. Teaching spontaneous responses to a young child with Down syndrome. Down Syndrome Research and Practice, [cited August 3, 2007]. [Open Access Full Text]
- Buckley, S. Literacy and language. In: Rondal JA, Buckley S, editors. Speech and language intervention in Down syndrome. London: Whurr; 2003. p.132-153.
- Halle JW. Teaching functional language to the handicapped: An integrative model of natural environment teaching techniques. Journal of the Association for Persons with Severe Handicaps. 1982;7:29-37.
- Rogers-Warren A, Warren SF. Mands for verbalization: Facilitating the display of newly trained language in children. Behavior Modification. 1980;4:361-382.
Acknowledgement
We are grateful to the families who devoted their time to this project and thank Developmental Disabilities Institute for providing partial funding for this research. We also thank Dr. Joe Reichle for providing scholarly critique of this manuscript.
Received: 4 August 2007; Revised version received: 14 June 2008; Accepted: 21 June 2008; Published online: January 2010

