Learning the hard way: Avoidance strategies in young children with Down syndrome
This paper overviews findings from a series of studies of cognitive development in children with Down syndrome aged between birth and 5 years. These studies provide evidence of the persistence and elaboration of a particularly inefficient learning `style' during these early years, one which affects both the acquisition and consolidation phases of learning. The ability levels demonstrated at very young ages were surprisingly high but instead of building on these skills, many children simply allowed them to deteriorate. Consolidation of new skills was compromised by poorly motivated performance on `easy' tasks while the avoidance strategies produced in response to `difficult' tasks resulted in many learning opportunities being missed. Implications of these findings are discussed and in relation to assessment, the importance of awareness of the inherent instability in developmental processes in children with Down syndrome is stressed.
Wishart, J. (1993) Learning the hard way: Avoidance strategies in young children with Down syndrome. Down Syndrome Research and Practice, 1(2), 47-55. doi:10.3104/reviews.10
Introduction
Down syndrome is the most common known cause of cognitive impairment in young children. It is a chromosome disorder which affects both mental and physical development in a number of detrimental ways and although advances in medicine have succeeded in alleviating many of the major associated health problems, little headway has yet been made in reducing the considerable learning difficulties encountered by most children born with this condition. While the present generation of children can confidently be expected to live much longer and healthier lives than children with Down syndrome born in earlier decades, it is still unfortunately the case that most will meet great problems in achieving many of the important milestones in early cognitive development (for overviews, see Gibson, 1978; Lane and Stratford, 1985; Cunningham, 1987; Cicchetti and Beeghly, 1990).
The majority of children born with Down syndrome - 95% - have standard trisomy 21, that is, they have three rather than the usual two copies of chromosome 21 in every cell of their body. This extra chromosome results in significant abnormalities in the architecture and functioning of the brain at birth and continues to compromise the growth of the brain throughout childhood and into adulthood. These limitations of the efficiency of the biologically-given 'tools' for cognition undoubtedly place some restrictions on what can be achieved by anyone with Down syndrome.
This does not mean that nothing can be done to help the children to overcome or compensate for some of the learning difficulties they inevitably must face. Although few direct benefits may come from the increased understanding of the neurological substrates of Down syndrome, development is always the result of a complex interaction between a child's genetic inheritance and the environment in which he or she grows and learns.
The fact that children with Down syndrome show huge differences in ability levels, with some being profoundly handicapped while others have moderate or occasionally only mild learning difficulties, demonstrates clearly that cognitive development in this group of children is not 'fixed' at birth. There are also few consistent findings that the IQs of children with Down syndrome are closely correlated with the IQs of their parents, further evidence that genetic factors alone do not determine the wide variations in learning ability reliably found in this population of children (Gibson, 1978; Hodapp and Zigler, 1990).
Why then are some children with Down syndrome so much more successful at learning than others? At present, the honest answer has to be that we do not know why such large individual differences exist. There has been no shortage of psychological studies of cognitive ability in children with Down syndrome but these have provided surprisingly few insights into the likely origins of these differences. Few families today do not receive the benefits of professional advice and early intervention programmes and in most developed countries full-time schooling is now the norm for all children with Down syndrome. This makes it unlikely that wide differences in ability levels stem simply from 'brighter' children having had more and better opportunities to learn than others.
There is another major gap in our understanding of developmental processes in Down syndrome - the reason behind the typical decline in the children's IQ scores as they grow older. This has been a robust finding from studies carried out over the years and disappointingly, recent studies indicate that early intervention has as yet failed to have any major impact on this decline (Sloper et al, 1986; Gibson and Harris, 1988; Wishart, 1991). The children continue to make steady developmental progress, but because the rate of progress is slower than ordinary children, their actual IQ score becomes lower over time - as IQ is worked out by comparison with age matched children each year. This slowing in developmental rate could be the product of psychological rather than biological processes, reflecting, for example, the cumulative effects of poorly-motivated learning, repeated failure to capitalise on new cognitive skills as they emerge in development, or a complex interaction between these two processes.
With this latter possibility in mind, this paper looks at how young children with Down syndrome approach the task of learning. In particular, it examines to what degree the children may be adding to their pre-existing difficulties by adopting behavioural strategies which undermine the progress of their learning.
The findings reported are drawn from a number of studies of early cognitive development carried out in Edinburgh over the last ten years. Full procedural details of these studies can be found in other publications (see below) and need not be repeated here. Instead, this paper will attempt to draw out some common themes from the studies. These studies have found consistent evidence that children with Down syndrome make poor - and sometimes very inappropriate - use of the skills they develop in early childhood; they also illustrate how the children often go to great lengths to avoid learning opportunities, the end result being that they may effectively be adding to their already-existing handicap in such situations.
Object concept studies
The clearest examples of the developmental patterns which have emerged from our research come from our studies of object concept development. Development of a concept of objects is a very important step in early cognitive development and one which in the 1970s and 1980s was the subject of more research attention than almost any other topic in developmental psychology. This particular sequence in early development has consequently been extensively described in very close detail (for overviews, see Schuberth, 1982; Harris, 1984; Wishart, 1992). This makes it easier to detect any fine-grain differences in how normally-developing children and children with Down syndrome may go about achieving their understanding of objects.
How do we define a 'concept of objects'? Psychologists typically give very complicated, jargon-ridden definitions drawn from a Piagetian theoretical framework. Basically, however, it refers to the fact that in order to to understand even the simplest of events, a child needs to acquire an understanding of physical reality and central to that understanding is learning the defining properties of objects. Children must learn, for example, that objects exist independently of their actions, and that they continue to exist even when they cannot see them or act upon them. They must also learn that every object has a unique identity - that two objects seen at different times which look identical are not necessarily one and the same object, for instance. They must come to appreciate that objects are subject to the laws of space, time, and causality - that is, that the same object cannot be in two places at one time, that any object must have contacted another to have caused its movement, that one object placed inside another will share in all of the movements of the first object, and so on.
This may all sound very far removed from dealing with everyday practical problems but imagine, for example, not being able to understand that when some object, say a key, is put inside something, say a box, and that box then moved, that the key will still be in that same box in its new location, even although it was not itself seen to move between the two places. Adults find it very surprising that children have to learn principles which are as basic as this but there is huge body of empirical evidence showing that children initially have very little understanding of these simple rules. Many psychologists, moreover, believe that the thinking processes underpinning object concept development are prototypical of all later thinking. Gaining a working understanding of objects and their properties is seen as an essential first step in early learning, one without which acquisition of many more advanced concepts would be impossible.
Research has shown that it takes the average, normally-developing child the first two years of life to attain a fully-developed concept of objects. This occurs in a sequence of six well-defined, hierarchical stages, first described by Piaget nearly fifty years ago (Piaget, 1936). Early work with children and adolescents with Down syndrome suggested that this process took very much longer for them to complete (Wohlheuter and Sindberg, 1975; Silverstein et al, 1975) and until relatively recently, few researchers even attempted to test infants with Down syndrome on object concept tests, the assumption being that if the older children had difficulty with these tasks, there was little point in trying them with infants.
Our research, however, focussed on children with Down syndrome aged from birth to 5 years old on the basis that although children at the youngest age levels could not be expected to succeed on most, or possibly even any, of the tasks to be presented, it was nevertheless important to know how young children with Down syndrome responded to these sorts of cognitive challenges (see also, Morss, 1983; Dunst, 1990).
How do we test children's understanding of objects?
The various tasks used to test which stage a child is at in object concept development are very similar to those routinely given to babies during developmental checks at the baby clinic. A hiding game is played, with the hiding sequence increasing in complexity according to the level of development being tested. A small, attractive toy is hidden, usually either inside a cup or under a small cloth. In the easiest task, only one cup or cloth is present but in all higher level tasks, the infant must choose correctly from one of two or more identical cups or cloths in order to find the hidden toy; unless he or she fully comprehends the particular hiding sequence, performance will only be at chance level. Although age of achievement of each developmental stage can vary enormously in individual children, very characteristic errors are commonly made in response to each level of task and it has been shown that these errors appear at some point in the development of all children in all cultures, regardless of their intelligence level.
The Edinburgh studies
A brief overview of findings from 4 interlinked studies of object concept development in children with Down syndrome will be given here. These are: a long-term longitudinal study of thirty children aged between birth and 3 years (Wishart, 1988, 1990, 1993), a related, shorter-term study with twelve 3-5 year olds (Wishart, 1987), a cross-sectional, test/re-test study of eighteen children aged 6 months to 4 years (Wishart and Duffy, 1990), and a small-scale training study with ten 1-3 year olds (Wishart, 1986). Findings from the long-term longitudinal study are given most space as this study provided the most interesting - and unexpected - insights into early developmental processes in children with Down syndrome.
In the main longitudinal study, performance on four different levels of object concept task was monitored (see Figure 1). The 4 tasks were presented in increasing order of difficulty, with four trials of each task being given. All children were tested fortnightly on all four tasks, regardless of their age or success/failure rates in previous sessions. Formal testing of the very youngest children did not commence until they could demonstrate the ability to reach out to a dangling object (this reaching did not need to be well-developed or highly skilled, only present).
Criteria for attributing success/failure on each level of task were drawn from an earlier cross-sectional study of object concept development in 228 normally-developing infants aged between 4 and 22 months (Wishart and Bower, 1984) and from a longitudinal training study in which 24 infants (again, normally-developing) had been tested regularly with object concept tasks from the age at which they could first reach (Wishart and Bower, 1985). To be credited with achievement of any given stage, children were required to pass all four trials of the appropriate level of object concept task in two consecutive testing sessions. These were strict criteria but given the limited number of possible hiding places in each task, it was essential to ensure that all passes were genuine and not likely to be attributable to chance success.
A total of 38 children with Down syndrome initially entered the study, ranging in age from birth to 3 years. Data from 5 children, all but one in the upper age range, had to be excluded from age of acquisition analyses since after three months of data collection, it was not possible to determine their exact cognitive status with any degree of confidence. Although these children were still producing errors on one or more tasks, they also scored clear passes on these same tasks in a number of sessions. This made it likely that these subjects were in the post-acquisition rather acquisition stage of the understanding required to pass these tasks (see below). Data collection from a further 3 children was interrupted by extended periods of hospitalisation or ill-health at what may have been critical periods. Development in the remaining 30 children was regularly monitored over periods of from 9 months up to 3 years, depending on each child's age on the first testing session and on his/her developmental status. All but one of these subjects provided data on at least one major stage transition in object concept development; most provided data on two transitions, while the youngest-entering children provided data on all four.
A primary aim of this study was to investigate whether cognitive development in children with Down syndrome could best be understood in terms of a slowed-down version of normal cognitive development or whether it is essentially different in nature from normal developmental processes. Many longitudinal studies of development in children with Down syndrome which have not included control groups in their design have confidently interpreted their findings within the framework of normal developmental theory. Some of the studies which have included some form of control group are no less problematic since the method of matching adopted, usually mental age scores from a norm-referenced test, has effectively prejudged this issue (see Duffy and Wishart, 1987; Wishart and Duffy, 1990). The problems of subject matching in empirical studies of children with known developmental problems is seldom directly addressed.
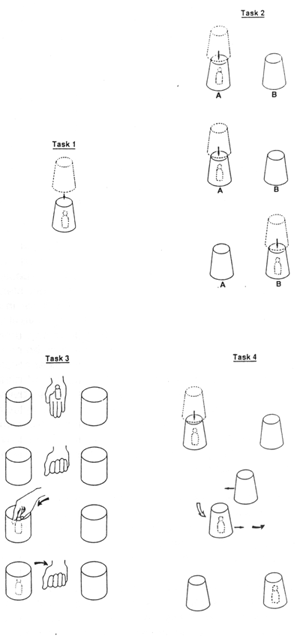
Figure 1. The object concept tasks
In this study, children with Down syndrome were initially matched with normally-developing children of the same chronological age but a second matching, based on developmental stage, was also carried out on completion of data collection. In this second retrospective matching procedure, individual records were examined for the age at which each child had first passed a given level of task to criterion and the performance of matched Down syndrome and non-Down syndrome children was then compared over a specific number of sessions prior to and subsequent to achievement of that particular stage in development. This method of matching, on the basis of transition points in acquisition of the object concept, allowed precise matching on specific tasks at specific points in development but left open the option that the process of cognitive development before and after acquisition of any given stage in object understanding might differ in the two groups of children.
Surprisingly high levels of ability - put to very inefficient use
Analyses of the learning patterns of the two groups produced some very intriguing results (see Table 1). As was to be expected, the normally-developing children outstripped their counterparts with Down syndrome in almost all aspects of performance, succeeding on each level of task consistently earlier and reliably demonstrating their new skills in all subsequent testing sessions. However, the cognitive ability demonstrated by many of the children with Down syndrome was much greater than might have been expected on the basis of ability levels previously reported for older children with Down syndrome tested on similar tasks (and initially found in the 3-5 year olds we ourselves tested - see below). Many of the infants with Down syndrome in this longitudinal study succeeded on one or more of the 4 levels of task while still within the normal age range for that task; a very few even succeeded in first passing some tasks at an earlier age than their non-handicapped control.
| AGE OF SUCCESS ON HIDING TASKS 1-4 | Task 1 | Task 2 | Task 3 | Task 4 | ||
|---|---|---|---|---|---|---|
| CHILDREN WITH DOWN SYNDROME | Mean Age (mths) | 7.75 | 10.50 | 19.25 | 18.0 | |
| Range | 6.25-10.75 | 7.25-14.0 | 14.5-26.75 | 11.0-25.25 | ||
| NORMALLY DEVELOPING CHILDREN | Cross-sectional normative data | Age at which 75% children passed (mths) | 5.0 | 10.0 | 15.0 | 22.0+ |
| Longitudinal data (control group) | Mean age (mths) | 4.75 | 7.75 | 12.25 | 14.5 | |
| Range | 4.0-5.75 | 4.75-8.5 | 9.25-14.25 | 10.25-17.0 | ||
| (all months rounded up to nearest 0.25) | ||||||
Although it could be argued that this success was only achieved by virtue of the extra experience given with these tasks, this does not in itself materially detract from the fact that many of these children proved capable of reaching these cognitive levels by these ages. It is important, though, to note the wide range in age of achievement of each of these steps in cognitive development in the group of children with Down syndrome, much wider than in the group of normally developing children. While mean age of achievement in the group with Down syndrome is highly encouraging, a significant number of children took very much longer to reach the same stage in understanding than others, more than a year longer in some cases. There were no immediately apparent reasons for these huge individual differences. Some of the children who proved to be the most able came from the least advantaged backgrounds and/or had additional secondary physical handicaps to deal with (e.g. severe heart disorder) while some of the least able on the face of it had every conceivable advantage and yet made very slow progress through each of the stages.
Regardless of age of first success, however, a major and consistent problem seemed to be the consolidation of each newly-acquired skill. At each stage in development, the successes of the children with Down syndrome proved to be highly unstable. Success to criterion may have been achieved at surprisingly early ages in many cases, but this success was poorly maintained over subsequent testing sessions. Not long after success had first been recorded on each level of task, errors soon reappeared.
Although the children still seemed to be interested in the tasks and continued to search for the hidden toy, they frequently made errors on tasks which should by then have been relatively easy for them; they would look surprised at these errors but would often not bother to correct them. The 'search' strategies they used were often very low-level, moreover - indiscriminately sweeping both cups off the table, or simply selecting the same cup on every trial, a strategy that was bound to fail as often as it would succeed. Hiding chocolate or a biscuit instead of the toy met with some success in restoring performance in the weeks immediately following acquisition of a given stage in object concept development but this tactic proved ineffective in many of the later testing sessions.
By then the poor performance of children with Down syndrome seemed to reflect a competence that had deteriorated beyond retrieval rather than merely inadequate motivation or insufficient attention to the task in hand. The normally-developing children, by contrast, were found to work hard at each level of task in most testing sessions, regardless of whether a given task was above or below their current developmental status. Once success had been achieved at any level, it was usually easily reproduced in all subsequent testing sessions. In the few instances where it was not, it was generally very clear from the child's behaviour that he or she had not been sufficiently interested to search with any great care; in such instances, the introduction of chocolate almost always led to an immediate and very obvious revival of enthusiasm, followed by quick and accurate search.
'Switching out' of learning
These differences in performance profiles in the two groups of children did not only affect the consolidation phases of learning. There were also significant differences in how they approached tasks which had not yet been mastered. While the normally-developing children were in general willing to have a go at all levels of tasks in almost all testing sessions, the children with Down syndrome typically seemed prepared to work hard only on tasks which fell within a very narrowly-defined cognitive range, those only slightly more or less difficult than their current stage in development.
As we have already seen, tasks which should have been 'easy' given earlier success rates were not fully engaged in later sessions and consequently were often failed. 'Difficult' tasks were also routinely poorly engaged in, however, although these were more likely to be actively avoided rather than just given incomplete attention. Children resorted to a variety of diversionary behaviours in their attempts to avoid participating in these more challenging tasks. As a result, they often failed by default, not because they had made an error but because they had refused to participate in the required number of trials. It is worth noting that this 'switching out' was not just produced in response to experience of failure: children were as likely to opt out immediately after a successful as after an unsuccessful attempt at finding the hidden object.
The avoidance behaviours produced in response to difficult tasks were highly varied but they had two common features: firstly, they were usually maintained until successful (i.e. until a given trial of any task had to be abandoned) and secondly, they frequently involved the misuse of the child's burgeoning social skills. One particularly common - and highly effective - strategy, for example, was to look up in mid-hiding sequence and to lock eye contact with the tester. This behaviour obviously considerably reduces the chances of finding the hidden toy at the first attempt. Children would in any case often not go on to search at all, despite the fact that there was a very limited number of possible hiding places, all within very easy reach. Many simply sat back, maintaining eye contact, smiling and refusing to do anything until the tester moved on to some other task.
Other diversionary ploys included hand-clapping, waving, slipping down under the table, making silly faces, or producing some 'party trick', such as mimicking the telephone ringing. These sorts of behaviours, while often very charming, are clearly very context-inappropriate and it is not difficult to see how the stereotype of children with Down syndrome as happy, affectionate but not very bright children has become well-entrenched (Wishart and Johnston, 1990).
Analysis of individual performance profiles confirmed a strong relationship between the production of avoidance behaviours on a given level of task and the child's current stage in development. A child could be working very well in a testing sessions but would suddenly 'switch out' when a new task was presented. The moment the task was changed, even although the new task might involve hiding the exact same toy, that same child would revert to enthusiastic attention and efficient search, making it very clear that the previous avoidance behaviours had been highly specific to one particular task and not simply due to fatigue or boredom effects, to basic attentional deficits, or to any loss of motivation to solve tasks involving hiding toys.
Our previous research has shown that the developmental sequence underlying object concept development is a closely-integrated, hierarchical one, with each new step in development building on the last. In the case of children with Down syndrome, their counterproductive responses to both 'easy' and 'difficult' tasks means not only that old skills are not being exercised but also that opportunities to acquire new skills are being missed, a combination which could perhaps explain the decline in their developmental rate with increasing age and also the steady increase in the gap in developmental progress made by children with Down syndrome and ordinary children as all the children grow older.
Performance on object concept tasks at older ages
The instability of successes in these young children with Down syndrome suggests strongly that they may have considerable problems in consolidating their learning. This interpretation fits with the developmental patterns which emerged from the shorter-term study carried out with older children, the 3 - 5 year olds (Wishart, 1987). This study compared level of object understanding in 12 children with Down syndrome and 12 normally-developing children of matched chronological age.
Object concept development is rarely tested in older children who have no developmental problems; it is a competence which is simply assumed to continue through into later years. It seemed important to confirm this directly, however, since the poor performance of children with Down syndrome on object concept tasks at later ages might have more do with the nature of the test materials than with the level of conceptual development the tasks are intended to tap: simple hiding tasks designed to be attractive to infants might simply be insufficiently interesting to engage the attention of older children, with or without developmental delay.
These concerns proved to be groundless. The non-delayed children we tested clearly found all 4 object tasks very easy and many indeed treated them with some degree of scorn and/or suspicion; they nevertheless searched accurately on all trials of all four tasks in the first testing session. In contrast, the performance of the 3-5 year olds with Down syndrome was very poor on all levels of task, in line with findings from previous cross-sectional studies using similar tasks with children with Down syndrome in the same age range.
Success/failure patterns on subsequent testing sessions proved a surprise, however. The scores of the children with Down syndrome increased dramatically over subsequent sessions whereas the success rate of the non-handicapped children was found to deteriorate significantly. Performance levels were in fact very similar in the two groups within a couple of months, with the children with Down syndrome actually out-performing the normally developing children latterly on the highest level tasks (see Table 2).
| GROUP/TASK | SESSION | ||||||
|---|---|---|---|---|---|---|---|
| 1 | 2 | 3 | 4 | 5 | 6 | ||
| CHILDREN WITH DOWN SYNDROME | Task 1 | 12 | 12 | 12 | 12 | 12 | 12 |
| Task 2 | 5 | 11 | 12 | 8(+2) | 11(+1) | 10(+1) | |
| Task 3 | 5 | 9 | 10 | 12 | 11 | 11 | |
| Task 4 | 2 | 3 | 4 | 4 | 5 | 7 | |
| Combined totals | 24 | 35 | 38 | 36(+2) | 39(+1) | 40(+1) | |
| NORMALLY - DEVELOPING CHILDREN | Task1 | 12 | 12 | 12 | 12 | 12 | 12 |
| Task 2 | 10(+1) | 10(+1) | 11(+1) | 9(+3) | 10(+2) | 10(+2) | |
| Task 3 | 11(+1) | 9(+2) | 10(+1) | 10(+1) | 10(+1) | 7(+2) | |
| Task 4 | 10 | 10 | 5(+1) | 6(+1) | 6(+1) | 5(+1) | |
| Combined totals | 43(+2) | 41(+3) | 38(+3) | 37(+5) | 38(+4) | 34(+5) | |
| Maximum N=12. Numbers in parentheses are numbers of additional children scored as failing deliberately | |||||||
A number of factors proved to be responsible for these contrasting performance patterns. In the case of the ordinary children, it was very clear from the accompanying comments that elaborate teasing often underlay their poor performance in later testing sessions, and not any drastic drop in ability. On the third testing session, for example, one 4 year old casually removed the wrong cup in Task 2 and without even checking that there was no toy there, he shook his head sadly and said (imitating his mother's voice perfectly) "This boy has absolutely no sense whatsoever". More often than not, correct search could easily be restored in the normally-developing children by cajoling them or by substituting chocolate for the toy in hidings.
It was not possible to judge whether teasing was similarly responsible for the initially poor performance of the children with Down syndrome. Because of the very low levels of expressive language, it was far less easy in their cases to determine whether their lack of success was also a case of 'won't do' rather than 'can't do' (Koegel and Mentis, 1985). Little about their behaviour would have justified giving them the benefit of the doubt though. Cajoling or bribery was also far less effective, suggesting that the majority of their failures in early sessions were indeed genuine. The improvement shown by this group within just two months, however, was quite remarkable, particularly given that this sequence of development normally takes two years to unfold in children without any learning disability.
Taking the results from the 1-3 and 3-5 year olds together, two conclusions can be drawn. Firstly, it would appear that very young children with Down syndrome have much higher levels of cognitive ability than might be predicted from the initial performance of older children with Down syndrome on these same cognitive tasks. Secondly, it would seem that consolidation of new learning may be a major problem for children with Down syndrome. When the extent and rate of improvement in performance over sessions in the older children is considered along with ages of initial success on each level of object concept task and the subsequent instability of these achievements in the younger children, the interpretation that the older group were re-acquiring the understanding necessary to pass these tasks is difficult to avoid. The speed with which successes were achieved suggests a re-tuning of earlier learning, learning which had been inadequately consolidated at the time of initial acquisition, rather than new learning.
Motor skills, motivational deficits and cognitive development
Two important differences in the developmental profiles from the main longitudinal study deserve some further attention at this point: the lag in achievement of success on the lowest level task, Task 1, and the reversal in order of difficulty of Tasks 3 and 4 (see Table 1).
Task 1 requires the child to retrieve an object which has been placed under a cup. As can be seen in Table 1, all control subjects could reliably pass Task 1 by 6 months of age but none of the children with Down syndrome were yet able to do so. Examination of test records and videorecordings quickly revealed a rather simple possible explanation for this difference. Few of the children with Down syndrome had been able to reach prior to 6 months: even if they had understood where to search for the toy, they would have had no way of demonstrating this knowledge. Once able to reach, success on Task 1 usually quickly followed in Down syndrome subjects. This suggests strongly that the marked delay in passing this level of task could well have been due to its motor requirements rather than to its conceptual demands being beyond the ability levels of the children with Down syndrome being studied.
Children with Down syndrome are often hypotonic at birth and the development of both gross and fine motor skills is typically delayed in most children. Several studies have shown a relative superiority of mental over motor development in the first few years in Down syndrome, with motor skills lagging behind mental scores by as much as 10 months in some children (see e.g. LaVeck and LaVeck, 1977). This degree of mismatch could lead to a serious underestimation of competence and of the readiness to acquire cognitive skills if the tests used to assess cognitive status have a significant motor component.
Many of the most popular tests of early intelligence implicitly assume possession of a matching level of proficiency in motor skills but the requirements of object concept tasks had initially seemed to make them highly suited for use with young children with Down syndrome: although children need to be able to search, they do not need to be capable of sitting unsupported (they sit on their mother's lap) and they do not need to be able to reach with any great skill (since only the directional intent of their reaches must be clear).
It is nevertheless evident that even these minimal motor requirements still exceeded those of the average 6 month old baby with Down syndrome and great caution is therefore needed in interpreting any 'delay' in age of achievement of this particular stage in conceptual development when tested by this route. Visually-directed search might be a more appropriate behavioural index of understanding in this group of children at these young age levels, although visual tracking behaviours can be much more time-consuming to analyse and more difficult to interpret than manual search patterns (see e.g. Wishart and Bower, 1985).
The other major difference in developmental profiles in the two subject groups, in age of achievement of success on Task 3 , cannot be so simply explained, especially given the performance of the children with Down syndrome on Task 4. Tasks 3 and 4 are both inference tasks involving the invisible displacement of an object (see Figure 1). In both tasks, the toy is hidden inside something and then moved to a new location.
In Task 3, the experimenter hides the toy in her hand, places her closed hand inside one of the cups, surreptitiously leaves the toy there, brings out her closed hand, and then invites the child to look for the toy. Typically, the child will first search the closed hand, the location where the toy was last seen, and on failing to find the toy there, has to infer where it must be, i.e. where the hand last was, inside the cup. Task 4 is conceptually similar to Task 3 in that the desired object is also moved unseen to a new location but in this invisible displacement, there is no 'trick' element: the cup in which the toy has been hidden is simply transposed with the other, identical cup (as in 'find-the-lady' games), and the child then invited to search.
Our previous cross-sectional research with normally-developing children had demonstrated that Tasks 3 and 4 form a true developmental hierarchy: that is, that children consistently pass Task 3 before Task 4 and if unable to pass Task 3, will also fail on Task 4. This developmental pattern held in the case of the ordinary children tested longitudinally in this study but not in the case of the children with Down syndrome and in this instance, no simple explanation based on differential motor skills can be offered.
By the age at which the average child was reliably passing Task 3, 12 months, all of the children with Down syndrome were reasonably competent reachers; most could already pass Task 2 by this age and a very few had even succeeded on Task 4, both tasks with essentially identical motor requirements to Task 3. The mean age of success for the Down syndrome group on Task 4 (18 months), although significantly behind the mean for control subjects, in fact compares very favourably with norms for this task drawn from cross-sectional studies of object concept development in normally-developing children.
Although it is known that repeated exposure to object concept tasks can lead to accelerated development (Wishart and Bower, 1985) and although clearly this effect was greater in normally developing children than in children with Down syndrome (see Table 1), it is nevertheless important to register that many of these children with Down syndrome managed to reach the levels of understanding required to succeed on this task more or less on time, no mean achievement given the very strict criteria adopted in this study and their inherent cognitive disadvantage.
The developmental picture for Task 3 was far less positive. Age of success in the children with Down syndrome was very much later than in control children and also well behind cross-sectional norms for this task. Task 3 was generally the last task to be solved by the group with Down syndrome and more avoidance behaviours were produced over the course of the study during presentations of this task than in either Tasks 1, 2 or 4. The children with Down syndrome clearly responded to this task in a very different way to ordinary children, possibly because of its 'trick' element .
In Tasks 1, 2 and 4, the laws of physical reality dictate where the toy will be found; this is true in Task 3 also, but the surreptitious actions of the tester mean that the child's first search, in an apparently reasonable place, the tester's hand, will not be successful and a second search is required. The normally developing children occasionally showed some initial evidence of being put off their stride by this temporary set-back but most quickly went on to search further; in subsequent trials, many clearly enjoyed the 'trick', sometimes even second-guessing the tester by going straight to the cup on later trials, without first bothering to check her hand. Children with Down syndrome, by contrast, were more likely to refuse to watch any further trials and used a variety of methods, positive and negative, to avoid having to take part in more presentations of Task 3.
Motivational deficits, developmental instability, and assessment
The poor engagement, avoidance strategies and unstable success described above pose considerable problems to assessment. Procedures for many developmental tests recommend ending testing at the first point at which a child clearly fails. In object concept testing, it would usually be very safe with normally-developing children to assume that any child who cannot, for instance, pass Task 2, would also be unable to pass either Tasks 3 or 4. Any such assumption would seem to be very unsafe in the case of children with Down syndrome and it is all too easy to see how children might be considered 'untestable' in many situations or might not be given the opportunity to show the full extent of their capabilities because of their poor performance on relatively low-level tasks.
We investigated this aspect more closely in a small cross-sectional test/retest study (Wishart and Duffy, 1990) which used the same 4 object concept tasks but also test items from the Bayley Scales of Mental Development, a very widely-used measure of early cognitive development. Eighteen children with Down syndrome took part, aged 6 months to 4 years. The two sets of tasks were presented in the same testing session, with testing repeated one to two weeks later using exactly the same procedures. Both qualitative and quantitative aspects of children's performance were found to differ significantly in these two sessions. Even when overall raw scores were very similar on the two occasions, closer inspection of performance profiles revealed very different patterns of successes and failures on both object concept tasks and the more wide-ranging Bayley test items.
The variability in performance profiles on the object concept tasks showed no simple pattern, either in terms of age or task level. Two thirds of the children tested - 12 out of 18 - showed unstable performance and all levels of task were affected. 'Switching out' behaviours were reliably associated with these reversals in success/failure rates, with inappropriate or stereotyped behaviour typically underlying the failure in one or other of the two sessions.
Bayley peformance showed a similar degree of instability, although if comparisons had been restricted to overall scores, this would not have been detected. The raw scores of many children were in fact very similar over the two occasions (in some cases, identical) but examination of item-item profiles showed up substantial changes in performance over the two sessions (see Table 3). Over half of these instances of test/retest difference could once again be traced back to a clear unwillingness to engage fully in the particular task in one or other session. This task avoidance took many forms, from simple refusals to attend in younger children to more elaborate diversionary behaviours in older children. As in the earlier object concept studies, these failures to engage could be linked to the relationship between the difficulty level of the task being presented and the child's stage in development at time of testing, with items at both the easy and difficult ends of the child's developmental range seeming most vulnerable to motivational fluctuations.
| AGE (mths) | TESTING SESSION MEAN SCORE (AE) | TOTAL NUMBER OF ITEMS VARYING OVER SESSIONS | ||
|---|---|---|---|---|
| 1 | 11 | Fail-to-pass | Pass-to-fail | |
| 6 | 55.3(4.5) | 53.3(4.5) | 12 | 19 |
| 12 | 77.3(7.0) | 75.6(7.0) | 10 | 15 |
| 18 | 100.0(11.0) | 99.7(11.0) | 11 | 13 |
| 24 | 109.0(13.0) | 108.7(13.0) | 16 | 16 |
| 36 | 131.3(19.0) | 130.3(19.0) | 12 | 15 |
| 48 | 142.3(22.0) | 142.3(22.0) | 13 | 13 |
| Totals | 74 | 91 | ||
| AE= age equivalent level (in months) | ||||
Can we compensate for these motivational deficits?
How easy it will be be to bypass the children's apparent inclination to avoid learning remains to be seen. The extended period required for successful acquisition of most skills and the high rate of failure inevitably experienced when first attempting to learn any new skill cannot be conducive to learning and it is perhaps not surprising that many children with Down syndrome soon show evidence of becoming very reluctant learners. We have tried a number of different techniques aimed at minimising these adverse effects but to date, these attempts have met with only limited success.
In one small-scale study with ten 1-3 year olds, we tried embedding Task 3 into a training procedure in which single trials of the standard task were preceded by two related but more simple search tasks which were designed to draw the child's attention to factors relevant to solution of the standard task (Wishart, 1986). An earlier study by Morss (1984) had found that restructuring the task in this way had led to improved performance in children with Down syndrome, although interestingly, it did not enhance performance in normally-developing children at the same stage in their development.
In our study, if strict statistical criteria for success were adopted, relatively few gains were registered by the children, either within or over sessions. Despite the simplified presentations, moreover, there was again evidence of avoidance behaviours. Younger subjects were more likely to 'switch out' than older ones (as would be predicted on the basis of our findings from other studies, the ages of these children with Down syndrome, and the difficulty level of Task 3) and once again, avoidance behaviours were produced irrespective of whether search on the immediately preceding trial had been successful or not.
There was, however, a marked improvement in the quality of the searches made by most of the children with Down syndrome over these training sessions, in that they extended their search to more locations, showed greater attention to the hiding sequence and were more precise in their search behaviour. It is possible that more extensive training might have paid better dividends. If the long-term aim of research into development in children with Down syndrome is to find ways of compensating for some of the deficits and delays normally associated with this condition, then any improvement in performance is worth following up, even if it is not reliably shown and even if it is insufficient to meet statistically-determined criteria for 'significant' improvement.
We have had some greater success in some of our other studies which have used errorless training techniques, but the longevity of these gains has not been impressive and new skills have typically failed to generalise successfully to other cognitive contexts (see Duffy and Wishart, 1987; Duffy, 1990). The changes seen in these studies at least demonstrate that intervention can have some effect and give us something to build on in future studies.
The mis-use of social skills to side-step learning
The evidence of a growing tendency in children with Down syndrome to use socially-based strategies to get out of participating in difficult learning is of particular concern. In everyday learning situations, it is easy to see how parents and teachers, knowing the children to have an inherent learning disability and expecting them to have difficulties in learning, might unwittingly reinforce this kind of behaviour and allow themselves to be diverted into setting aside teaching for the moment and moving on to some more agreeable task, thereby.
The social skills of children with Down syndrome are often seen as their major asset and given the guaranteed presence of significant difficulties in other areas, it is not surprising that many parents concentrate on encouraging the acquisition of such skills. Overemphasis on the development of compensatory social skills may have the potential to do more harm than good however, given the inappropriate use clearly being made of these skills by many of the children in our studies. It may therefore be important to be aware of the possibility that such behaviours may have a hidden agenda in learning contexts and to take care not to aiding and abetting children in their efforts to side-step learning.
In Conclusion
The pressures of real life mean that even the best-intentioned parents sometimes often have to help their child to do something even although they feel that he or she could probably manage on their own given enough time. Trying to convince the child with Down syndrome that making an effort is worthwhile can also be a very uphill job in many instances, even when time is unlimited. At the very least, research such as that reported here should alert parents to the fact that from a very early age, children with Down syndrome may sometimes put as much effort into avoiding learning as into taking part in it and can therefore be putting themselves unnecessarily at further cognitive disadvantage.
Finding ways around this behaviour is going to require considerable ingenuity. This ingenuity is more likely to come from parents and teachers than from researchers. People who play a large part in the day-to-day lives of children with Down syndrome obviously have far more opportunities to observe the specific strategies that individual children develop to avoid difficult learning and to detect the particular situations in which they are most like to resort to such strategies.
Avoidance strategies are an understandable response to the high levels of failure the children may initially experience in most new learning situations but they may also be influenced by the low expectations adults often have of children with Down syndrome in situations which are cognitively-demanding. If this is the case, it might be possible to prevent avoidance strategies from becoming an established feature of the child's 'natural' learning style by paying greater attention to the psychological environment in which we expect children with Down syndrome to learn. With judicial management of learning experiences, it may even be possible to prevent such strategies from emerging in the first place, although limiting their effects is perhaps a more realistic objective. To do this will require a real partnership between parents, teachers, and researchers working in this field and a pooling of their respective expertises.
Acknowledgements
The research reported in this paper was supported by MRC Project Grants G87038755N/G9011079N. Thanks are extended to the mothers and children who participated in the studies, and to the teaching staff of Lothian Region schools, all of whom generously - and uncomplainingly - gave up their time to help with this research. The co-operation of the Scottish Down Syndrome Association and Lothian Health Board is also gratefully acknowledged.
References
- Carr, J. (1985) The development of intelligence. In D. Lane & B. Stratford (Eds.) Current Approaches to Down Syndrome (pp.167-186) London: Holt, Rinehart & Winston.
- Chumakov, I., Rigault, T., Guillou, S. et al. (1992). Continuum of overlapping clones spanning the entire human chromosome 21q. Nature, 359, 380-387.
- Ciccetti, D. and Beeghly, M. (1990) Children with Down Syndrome: A Developmental Perspective. Cambridge, England: Cambridge University Press.
- Cunningham, C.C. (1987) Early intervention in Down syndrome. In G. Hosking & G. Murphy (Eds.) Prevention of Mental Handicap: A World Review (pp. 169-182) London: Royal Society of Medicine.
- Duffy, L. (1990) The relationship between competence and performance in early development in children with Down syndrome. Unpublished Ph.D. dissertation, University of Edinburgh.
- Duffy, L. and Wishart, J.G. (1987) A comparison of two procedures for teaching discrimination skills to Down syndrome and non-handicapped children, British Journal of Educational Psychology, 57, 265-278.
- Dunst, C.J. (1990) Sensorimotor development of infants with Down syndrome. In D. Cicchetti & M. Beeghly (Eds), Children with Down Syndrome: A Developmental Perspective (pp.180-230). New York: Cambridge Univ. Press.
- Gibson, D. (1978). Down Syndrome: The Psychology of Mongolism. Cambridge, England: Cambridge University Press.
- Gibson, D. and Harris, A. (1988) Aggregated early intervention effects for Down syndrome persons: patterning and longevity of benefits. Journal of Mental Deficiency Research, 32,1-17.
- Harris, P.L. (1984) The development of search. In P. Salapatek & L.B. Cohen (Eds.), Handbook of Infant Perception. New York: Academic Press.
- Hodapp, R.M. and Zigler, E. (1990). Applying the developmental perspective to individuals with Down syndrome. In Cicchetti & Beeghly (Eds.) Children with Down Syndrome: A Developmental Perspective (pp.1-28). Cambridge, England: Cambridge University Press.
- Lane, D. and Stratford, B. (1985). Current Approaches to Down Syndrome. London: Holt, Rinehart & Winston.
- LaVeck, B. and LaVeck, G.D. (1977) Sex differences among young children with Down syndrome, Journal of Pediatrics, 91, 767-769.
- Morss, J.R. (1983) Cognitive development in the Down Syndrome infant: Slow or different? British Journal of Educational Psychology, 53, 40-47.
- Morss, J.R. (1984). Enhancement of object permanence in the Down Syndrome infant. Child: Care, Health & Development, 10, 39-47.
- Patterson, D. and Epstein, C.J. (1990) Molecular Genetics of Chromosome 21 and Down Syndrome. New York: Wiley-Liss.
- Piaget,J. (1953) The Origins of Intelligence in Children. London: Routledge and Kegan Paul (original French edition, 1936 ).
- Schuberth, R.E. The infant's search for objects: Alternatives to Piaget's theory of object concept development. In L.P. Lipsitt (Ed.), Advances in Infancy Research (Vol 2), 137-182. Norwood, N.J.: Ablex (1982).
- Silverstein, A., Brownlee, L., Hubbell, M. and McLain, R. (1975) Comparison of two sets of Piagetian scales with severely and profoundly retarded children. American Journal of Mental Deficiency, 80, 292-297.
- Sloper,P., Glenn, S.M. and Cunningham, C.C. (1986) The effect of intensity of training on sensori-motor development in infants with Down syndrome. Journal of Mental Deficiency Research, 30, 149-162.
- Wishart, J.G. (1986) The effects of step-by-step training on cognitive performance in infants with Down syndrome. Journal of Mental Deficiency Research, 30, 233-250.
- Wishart, J.G. (1987) Performance of 3-5 year old Down syndrome and non-handicapped children on Piagetian infant search tasks. American Journal of Mental Deficiency, 92, 169-177.
- Wishart, J.G. (1988) Early learning in infants and young children with Down syndrome. In L. Nadel (Ed.), The Psychobiology of Down Syndrome (pp.1-50). Boston: M.I.T. Press.
- Wishart, J.G. (1990) Learning to learn: the difficulties faced by infants and young children with Down Syndrome. In W.I. Fraser (ed.), Key Issues in Research in Mental Retardation (pp. 249-261). London: Routledge.
- Wishart, J.G. (1991) Early intervention. In W.I. Fraser, R. MacGillvray & A. Green (eds.), Halla's Caring for People with Mental Handicap: 8th ed. (pp.21-27). London: Butterworth Heinemann.
- Wishart, J.G. (1992) Acquisition of the object concept. In: L.R. Squire (ed.), Encyclopedia of Learning and Memory (pp. 489-492). New York: Macmillan.
- Wishart, J.G. (1993) The development of learning difficulties in children with Down syndrome. Journal of Intellectual Disability Research, 37 (in press).
- Wishart, J.G. and Bower, T.G.R. (1984) Spatial relations and the object concept: a normative study. In: L.P. Lipsitt & C.K. Rovee-Collier (eds.), Advances in Infancy Research: Vol.3. (pp. 57-123). Norwood, New Jersey: Ablex.
- Wishart, J.G. and Bower, T.G.R. (1985) A longitudinal study of the development of the object concept. British Journal of Developmental Psychology, 3, 243-258.
- Wishart, J.G. and Duffy, L. (1990) Instability of performance on cognitive tests in infants and young children with Down syndrome. British Journal of Educational Psychology, 59, 10-22.
- Wishart, J.G. and Johnston, F. (1990) The effects of experience on attribution of a stereotyped personality to children with Down syndrome. Journal of Mental Deficiency Research, 34, 409-420.
- Wohlheuter, M. and Sindberg, R. (1975) Longitudinal development of object permanence in mentally retarded children. American Journal of Mental Deficiency, 79, 513-518.

