The role of parents in early motor intervention
In this article we discuss the results of a motor intervention study that we conducted with young children with Down syndrome and other disabilities (Mahoney, Robinson & Fewell, 2001). Results from this study indicated that neither of the two major treatment models that are commonly used with young children with motor impairments was effective at enhancing children's rate of motor development or quality of movement. These findings add to an increasing body of literature indicating that early motor intervention procedures are not adequately meeting the goals envisioned for this endeavour. We argue that there are at least two interrelated reasons why this may be occurring. The first is that parents, who are the people with the greatest opportunities to promote children's motor learning, are not being asked to become active participants in their children's motor intervention. The second is that contemporary models of motor intervention have been focusing on motor learning activities that are incompatible with contemporary theories and research on early motor learning.
Mahoney, G, and Perales, F. (2006) The role of parents in early motor intervention. Down Syndrome Research and Practice, 10(2), 67-73. doi:10.3104/reviews.307
The clinical procedures that are dominating contemporary early motor intervention services for young children with Down syndrome and other disabilities have not been effective at addressing this problem. We maintain that there are at least two interrelated reasons why this may be occurring. The first is that parents, who are the people with the greatest opportunities to promote children's motor learning, are not being asked to become active participants in their children's motor intervention. The second is that contemporary models of motor intervention have been focusing on motor activities that are incompatible with contemporary theories and research on early motor learning. The purpose of this paper is to present research findings and theoretical arguments that support these positions.
The effectiveness of contemporary motor intervention services
In a recent article (Mahoney, Robinson & Fewell, 2001) we reported the results from a 12 month investigation of the effects of motor intervention on young children with motor delays. Our primary purpose was to understand the impact of the two most commonly used motor intervention methods as they were implemented in typical practice as opposed to controlled experimental conditions. We followed a group of 50 one year old children (M CA = 14.1 months). Each of these children were currently receiving motor intervention services from community based early intervention or therapy programs that identified their treatment models as being based upon either the Neurodevelopmental Treatment (NDT) (Bobath & Bobath, 1964, 1984; Butler & Darrah, 2001) or Developmental Skills ( Folio & Fewell, 2002) intervention models. For each treatment model our sample included both children with Down syndrome (n=27) and children with cerebral palsy (n=23).
To assess the impact of intervention on children's rate of motor development, we administered the Peabody Gross Motor Development Scale (Folio & Fewell, 1983) at the beginning and end of intervention. On average, children had motor development quotients of 49 at the beginning of intervention (55 for children with Down syndrome; 42 for children with cerebral palsy) and 48 after one year of intervention (51 for children with Down syndrome; 44 for children with cerebral palsy). There were no significant pre- post differences in motor development quotients between children with Down syndrome versus children with cerebral palsy, nor between children who received NDT versus children who received Developmental Skills treatment.
We computed a Proportional Change Index (PCI: Wolery, 1983) to examine how children's rate of motor development during intervention compared to their rate of development prior to intervention. For the entire sample the average PCI was 1.00. This indicated that the average motor development rate children attained during intervention was equivalent to their rate of development prior to intervention. However, the distribution of PCI scores indicated considerable variability in developmental rate changes. During intervention, 44% of the children decreased their rate of motor development by more than 10%, 32% maintained their rate of development within a range of plus or minus 10%, while 24% increased their rate of development by more than 10%. This pattern of developmental change did not vary significantly as a function of the type of intervention model children received or children's diagnosis (cerebral palsy vs. Down syndrome). While NDT produced slightly better PCIs than the Developmental Skills interventions (1.08 for NDT; 0.92 for Developmental Skills), these differences were not statistically significant.
We also assessed changes in the quality of children's movement by using items from The Infant Motor Evaluation (TIME: Miller & Roid, 1994) to rate several components of movement from videotaped observations of children in multiple positions at the beginning and end of intervention. Because this use of the TIME was not a standardised procedure, we were unable to determine how observed changes in quality of movement compared to changes that might be expected due to maturation. However, our quality of movement findings were generally consistent with our results for children's rate of development. During intervention, the group of children as a whole improved their quality of movement, but only at a level consistent with their quality of movement at the beginning of intervention. In general, improvements were equivalent for children with Down syndrome and children with cerebral palsy regardless of whether they received the NDT or Developmental Skills treatment models.
Consistent with findings from previous studies (Bower, Michel, Burnett, Campbell & McLellan, 2001; Harris, 1997; Palmer, 1997; Palmer, Shapiro, Wachtel et al., 1988), results from our study present a sobering picture of the benefits that infants with Down syndrome and cerebral palsy attain from participating in motor intervention. Whether children received services based upon the NDT or Developmental Skills treatment models, on average their rates of motor development did not change during intervention. Our results add to the accumulating evidence that the treatment methods currently used in early motor intervention are weak at best, and fall far short of the hopes and vision upon which this endeavour was originally based (Ketelaar, Vermeer, 't Hart van Petegem-van Beek & Helders, 2001; Rothberg, Goodman, Jacklin & Cooper, 1991; Weindling, Hallam, Gregg, Klenka, Rosenbloom & Hutton, 1996). These results suggest that there is a crisis in the lack of evidence for the efficacy of motor intervention. They demand that this field launch thoughtful and aggressive efforts to develop, evaluate and integrate more effective treatments into practice.
Reasons for the lack of effectiveness of contemporary motor intervention procedures
We believe that there are at least two major reasons why motor intervention may be so ineffective. The first is related to the way that service providers work with parents. The second is related to the appropriateness of the learning activities that are emphasised in motor intervention. In the following we discuss each of these issues.
How motor interventionists worked with parents and children
One of the questions we examined in our study was how did interventionists work with parents. We conducted two analyses to attempt to address this question. First, we asked providers to maintain a log of the services they provided to children. Among other questions, the log asked interventionists to indicate:
(1) whether parents were present when their child received motor intervention services;
(2) whether interventionists provided parents with suggestions to follow through with at the end of the session; and
(3) if interventionists provided suggestions, what was the nature of these recommendations.
Second, we videotape recorded pre- and post- intervention observations of parent-child interaction. We assumed that if interventionists had been effective at providing parents with information and suggestions that were relevant to their children's motor development, this would be reflected in changes in the way that parents interacted with their children.
Findings from the intervention service logs indicated that interventionists provided services to children an average of 35 times over a 12 month period. On average these sessions were 50 minutes long. Parents were present in only 57% of these sessions, or approximately 1.5 sessions per month. On a monthly basis, the average amount of time parents spent observing their children's intervention sessions was one hour and twenty minutes, and the number of recommendations parents received was fewer than two. The majority of the recommendations that parents were given were related to teaching specific motor skills or to helping their child with tone, posture or alignment. Fewer than one half of these recommendations were related to parents encouraging or supporting their children's movement in the natural environment.
Parent-child observations were coded using the Maternal Behavior Rating Scale (Mahoney, 1992). Comparison of the pre- and post- observations indicated that intervention had no affect whatsoever on the way parents interacted with their children.
In general, our findings related to parent involvement were astonishing, particularly given the very young age of the children in this study and the fact that none of them were even walking when intervention began. Parents were only present to observe their children's intervention in little more than one half of the sessions that took place during this study. While interventionists did provide suggested activities that parents could do to support their children's motor development, the number of suggestions that were provided was extremely small.
During the past several years, a number of articles have been published related to parent involvement in motor intervention. These articles have argued that parents should play a more central role in motor intervention (Darrah, Law & Pollack, 2001); provided data indicating that parents are comfortable with this role (Sayers, Cowden & Sherrill, 2002); and demonstrated that parent involvement can have a positive impact on motor intervention effectiveness (Hamilton, Goodway & Haubenstricker, 1999; Ketelaar, Vermeer, Helders & Hart, 1998; Torres & Buceta, 1998).
However, given the low level of effort that went into to parent involvement in our study, it is not surprising that intervention had no effect on parent-child interaction or that parent participation did not affect intervention outcomes. It was our impression that although the interventionists who participated in this study did work with parents, they did not treat parents as central participants in their children's motor intervention programme. Rather, the majority of interventionists acted as if they believed that motor intervention is a service that takes place primarily between them and the child. They appeared to view parent participation as an optional activity that merely augmented the services that they themselves provided the child.
What is the most important thing for children to do to enhance their level of motor functioning?
In our study we compared the effectiveness of Neurodevelopmental Treatment and Developmental Skills which are arguably the two most influential motor intervention approaches that have been used with young children over the past 30 years. NDT was developed in England for treatment of children with cerebral palsy as well as adults who experienced stroke (Bobath & Bobath, 1964; 1984). It involves handling children to inhibit abnormal tone and facilitate automatic reactions, such as righting and equilibrium, to promote normal movement patterns (Bly, 1983; 1991). It attempts to mitigate underlying impairments in the central nervous system by guided practice of typical motor patterns (Butler & Darrah, 2001).
Developmental Skills interventions focus on the learning and mastery of normally sequenced motor milestones, with intervention targets identified from skills at the next higher level (e.g., Hanson & Harris, 1986). Instructional strategies tend to be behavioural in nature, i.e., children are encouraged to engage in exercises or structured play activities that target specific skills. The Developmental Skills approach assumes that children will attain higher levels of motor development and independent functioning through guided practice and reinforcement. This approach is reflected in several commonly used early intervention scales and accompanying domain-specific curricula. Examples include, the Portage Guide to Early Education Program (Bluma, Shearer, Froman & Hiliard, 1976); the Hawaii Early Learning Profile (Furuno, O'Reilly, Hosaka, Inatsuka, Zeisloft-Falbey & Allman, 1998); and the Peabody Developmental Motor Scales (Folio & Fewell, 2002).
These two intervention models are very different in terms of what they consider to be the most important behaviours to address during intervention sessions. Since NDT focuses on quality of movement, presumably NDT is based on the assumption that children's experience or ability to engage in normal movement helps to enhance their rate of motor learning or development. In contrast, the Developmental Skills approach focuses on teaching higher level motor skills that children have not yet mastered. This approach is based upon the assumption that children's motor functioning will improve as they learn the motor skills that children who have higher levels of motor proficiency typically perform. However, the NDT and Developmental Skills approaches, are similar to each other insofar as the behaviours that are the focus of intervention demand that interventionists provide children with considerable amounts of physical support, since children are unable to independently perform the motor behaviours being targeted.
It is interesting to note, however, that the motor behaviours that both of these intervention models consider to be critical to children's motor learning and development are not the behaviours that contemporary research is reporting to be the factors that enhance children's early motor learning. Much of contemporary motor development research is evolving from Dynamic Motor Theory (Thelen & Ulrich, 1991). This theory postulates that motor development results from children constructing solutions to motor problems. Children develop new motor behaviours by using their unique characteristics and capacities to explore situations through which they discover new and more adaptive forms of gross motor behaviour. To accomplish this, infants must attend to the information generated by their own bodies as well as to the information available in the context. Dynamic Motor Theory highlights the importance of child-initiated motor activity, and emphasises that repeated practice and exploration of motor movements plays a major role in the acquisition of more adaptive motor behaviours.
Adolph and her colleagues from New York University (See Adolph & Berger, in press) have reported findings from several studies on factors that affect the motor learning of infants and toddlers that are highly supportive of Dynamic Motor Theory. In one study Adolph, Vereijken and Denny (1998) investigated how infants' age (e.g., neurological maturation), body dimensions and motor experience influenced the quality of children's crawling from their first attempts at crawling until they began walking. Results indicated that children's age and body dimensions alone could not account for the speed and efficiency of later forms of crawling. However, the amount of experience children had using early crawling patterns (e.g., belly crawling) was the best predictor of the speed and efficiency with which children attained the more advanced form of crawling using their hands and knees.
In another study Adolph, Vereijken and Shrout (2003) conducted an investigation designed to determine what changes in the development of toddlers' walking, and what are the factors that contribute to these changes. They compared how children's body dimensions, age and walking experience influence the walking proficiency of infants and toddlers. Results indicated that as children become bigger, older and more experienced their steps become longer, narrower, straighter and more consistent. To examine the factors that contribute to these changes they used measures of children's body dimension, age and experience as predictors of their level of walking skill. Results indicated that when all three of these variables are analysed at the same time, the amount of experience that children have walking is the only significant predictor of the rate that they improve their ability to walk.
To illustrate what experience actually means and why this is such a major influence on the development of children's walking, Adolph et al. (2003) described several observations that they had made in prospective diaries they kept on children who were learning to walk. According to these investigators:
"Infants' everyday experiences with locomotion occur in truly massive doses, reminiscent of the immense amounts of daily practice that promote expert performance in world class musicians and athletes. … walking infants practice keeping balance in upright stance and locomotion for more than six accumulated hours per day. They average between 500 and 1500 walking steps per hour so that by the end of each day, they may have taken 9,000 walking steps and traveled the length of 29 football fields".
"infants' walking experience is distributed throughout their waking day, with short periods of walking separated by longer rest periods where infants stand still or play"…..infants' intermittent experience with locomotion within the course of each day and across their first few months of walking may provide them the time to consolidate learning and to allow fatigue and flagging motivation to dissipate".
"infants' everyday walking experiences occur in a wide variety of events, places and surfaces. … the variety of everyday walking experience resembles variable and random practice schedules …. (that) lead to a process of continually generating solutions anew". (Adolph, Vereijken & Shrout, 2003, p 494-495)
Based upon their research findings as well as these dramatic observations, Adolph et al. (2003) conclude that the magnitude and diversity of experience children have in engaging in spontaneous or self initiated movement lies at the heart of motor learning and developmental change.
We believe that the conclusions from this line of research challenge the focus of the practices that have dominated contemporary motor intervention practice. They suggest that the key to promoting children's rate of motor development are not the sporadic episodes of professionally dominated intervention activities that are focused on getting children to experience normal motor movement or to learn higher level motor skills. Rather these research findings suggest that the key to enhancing motor learning is to maximise children's level of spontaneous motor activity throughout their daily routine. The challenge for all children with motor delays is to encourage them to engage in the amount of crawling or walking that typically developing children do during the process of motor learning. This might mean that intervention will need to help children with Down syndrome and other conditions who are learning to walk to "average between 500 and 1500 walking steps per hour so that by the end of each day, they take 9,000 walking steps and travel the length of 29 football fields" Adolph, Vereijken & Shrout, 2003, p. 494).
Who has the greatest potential to maximise children's motor experience? Reconsidering parent involvement
The question remains, do parents have the capability of meeting the challenge described above of maximising their children's level of motor activity? We believe that this is a question that can only be answered as researchers move forward with testing the viability of this type of motor intervention model. Nonetheless, it is important to emphasise that we will never be able to maximise children's level of motor activity so long as the field of motor intervention continues to implement the types of sporadic, professionally dominated services that we observed in our study.
To illustrate this point, we have conducted a hypothetical analysis of the opportunities therapists have to directly influence children's motor development compared to the opportunities that parents might have. For this illustration, we used data obtained from our own study indicating that on average therapists provide 35 intervention sessions to children even when services are scheduled to occur once a week throughout the entire year. As we also observed in our study, we assumed that each of these sessions last approximately 50 minutes. We then compared this to the amount of opportunities parents have to impact their children's motor development. Our calculations for parents were based upon the assumption that parents spend only one hour a day in one-to-one contact with their children. When we examine the total amount of time that therapists have to interact with a child each week, we estimate that in a fifty minute session, approximately 45 minutes can be spent in one-on-one contact with the child. This can be compared to parents who spend 420 minutes with their child each week.
However, since parents are with their children 52 weeks each year, while therapists average 35 weeks, the greater amount of one-to-one time parents spend with their children each week is magnified by the number of weeks they are with their children. Assuming that most adults engage in 10 interactions per minute, parents engage in at least 220,000 discrete interactions with their children each year, while motor intervention professionals engage in only 15,750 interactions in the same period of time.
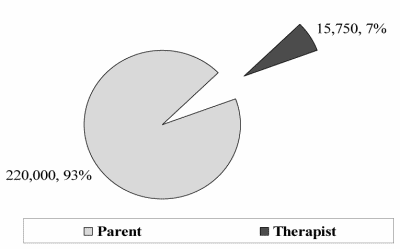
Figure 1 | Who has the greatest potential to maximise children's motor experience?
As illustrated on Figure 1, if a child were scheduled to receive motor therapy once each week, in one year parents would have at least 200,000 more interactions, or opportunities to influence their children's motor activity, than would therapists.
This is an extremely conservative estimate of the opportunities parents have to influence their children's development. If parents spend two, three or more hours each day interacting with their children, as many parents do, the discrepancy between the opportunities parents have to interact with their children compared to the opportunities of therapists would be magnified by 2 or 3 times. Still, this example illustrates how even parents who have limited time to be with their children because of work or other responsibilities, still have substantially more opportunities to influence their children's development than professionals could ever have. These data point out that if the key to children improving their motor learning and development is the amount of motor activity they engage in each day, effective intervention will not occur unless parents are asked to play a major role in this endeavour.
How do we maximise children's level of spontaneous motor activity?
Given that motor activity is the key to promoting children's motor learning, the challenge we are faced with is how to maximise children's spontaneous motor movement. To this end, there are two developments that are worth considering. The first is the work of Ulrich and his colleagues (Ulrich, et al., 2001). These researchers investigated the effects of spontaneous stepping practice on the rate that children with Down syndrome learned to walk (Ulrich, et al., 2001). In addition to receiving traditional physical therapy, parents provided their children with practice stepping five days a week for eight minutes each day by supporting them on specially engineered miniature treadmills. Results indicated that the spontaneous stepping practice helped children with Down syndrome walk independently approximately 100 days sooner than the children who did not receive the treatment. One important question raised by these findings is that if such robust effects can occur when children receive only modest (8 minutes per day) amounts of arranged practice, what would happen if we could enhance children's spontaneous activity throughout their daily routines?
The second line of research is related to findings from relationship focused early intervention studies. There is an increasing body of evidence that when parents are taught to interact more responsively with their young children with developmental disabilities (including Down syndrome) (McCullom & Hemmeter, 1997), children make dramatic improvements in their cognitive, language and social emotional functioning. The rationale for this approach to intervention has come from the numerous studies reported in the child development literature that have demonstrated positive relationships between responsive parenting and children's development. In a recent series of studies, we reported findings that suggest that the effects of parental responsiveness are mediated by the impact that this style of interaction has on children's spontaneous activity (Mahoney, Kim & Lin, in press; Mahoney & Perales, 2003; 2005). When parents are taught to interact more responsively, their children are more apt to engage in a number of spontaneous behaviours including attention, persistence, initiation, and exploration.
While it has yet to be determined how parental responsiveness effects the motor development of children with delayed motor development, research reported by Hanzlik and her colleagues suggests that responsive interaction may also be an effective intervention for enhancing the spontaneous movement of these children (Hanzlik & Stevenson, 1986; Okimoto, Bundy & Hanzlik, 2000). This research suggests that young children with cerebral palsy engage in greater amounts of spontaneous play and motor activity when their mothers interact responsively rather than directively with them. This remains an important line of research to pursue, particularly since relationship focused interventions can be easily integrated into the daily routines that parents have with their children, without placing undue stress on parents.
Summary
In this article we discussed how recent motor intervention research suggests that the intervention procedures that have dominated contemporary motor intervention practice with children with Down syndrome and other disabilities have not been effective at enhancing children's motor functioning. We proposed two reasons for the ineffectiveness of contemporary methods. The first is that parents have not played a major role in carrying out motor intervention activities with their children; the second, is that motor intervention may be targeting behaviours that have little to do with enhancing motor learning. We reviewed contemporary theory and research which suggest that the key to motor learning is the amount of spontaneous motor experience that children have. We discuss some recent research which has shown dramatic improvements in the rate that children with Down syndrome children learn to walk independently by providing children with minimal amounts of spontaneous stepping practice. Finally, we suggest that this approach to intervention may be enriched by examining ways that parents can promote their children's level of motor movement throughout the daily routine.
Correspondence
Gerald Mahoney, Ph.D • Verna Houck Motto Professor of Families and Communities, Mandel School of Applied Social Sciences, Case Western Reserve University, 10900 Euclid Avenue, Cleveland, Ohio 44106 • Tel: 216-368-1824 • E-mail: gerald.mahoney@case.edu
References
- Adolph, K.E. & Berger, S.E. (in press). Motor development. In D. Kuhn & R.S. Siegler (Eds.). Handbook of child psychology. Vol 2: Cognition, perception and language (6 th ed.) New York: Wiley.
- Adolph, K.E., Vereijken, B. & Denny, M.A. (1998). Learning to crawl. Child Development, 69(5), 1299-1312.
- Adolph, K.E., Vereijken, B. & Shrout P.E. (2003). What changes in infant walking and why? Child Development 74(2), 475-497.
- Bly, L. (1983). The components of normal movement during the first year of life and abnormal motor development. Chicago, Il, Neurodevelopmental Treatment Association.
- Bly, L. (1991). Historical and current view of the bases of NDT. Pediatric Physical Therapy, 3, 131-135.
- Bluma, S., Shearer, M., Frohman, A. & Hilliard, J. (1976). Portage guide to early intervention manual. Portage, WI: Portage Project.
- Bobath, K. and Bobath, B. (1964). The facilitation of normal postural reactions and movements in the treatment of cerebral palsy. Physiotherapy, 80, 246-262.
- Bobath K. and Bobath, B. (1984). Motor development in the different types of cerebral palsy. London, England: Heinemann.
- Bower, E., Michel, D., Burnett, M., Campbell, M.J. & McLellan, D.L. (2001) Randomized controlled trial of physiotherapy in 56 children with cerebral palsy followed for 18 months. Developmental Medicine and Child Neurology, 43 , 4-15.
- Butler, C. & Darrah, J. (2001). Effects of neurodevelopmental treatment (NDT) for cerebral palsy: An AACPDM evidence report. Developmental Medicine and Child Neurology, 43, 778-790.
- Darrah, J., Law, M. & Pollack, N. (2001). Family centered functional therapy-A choice for children with motor dysfunction . Infants and Young Children, 13(4), 79-87.
- Folio, M.R. & Fewell, R.R. (1983). Peabody Developmental Motor Scales. Austin, TX: Pro-Ed.
- Folio, R.M. & Fewell, R.R. (2002). Peabody Developmental Motor Scales (PDMS-2). Austin, TX: Pro-Ed.
- Furuno, S., O'Reilly, K.A., Hosaka, C.M., Inatsuka, T.T., Zeisloft-Falbey. B. & Allman, T. (1998). Hawaii Early Learning Profile. Palo Alto, CA.: Vort.
- Hamilton, M., Goodway, J. & Haubenstricker, J. (1999). Parent-assisted instruction in a motor skill programme for at-risk preschool children. Adapted Physical Activity Quarterly, 16(4), 415-426.
- Hanson, M.J. & Harris, S.R. (1986). Teaching the young child with motor delays: A guide for parents and professionals. Austin, TX.: Pro-Ed.
- Hanzlik, J.R. & Stevenson, M.A. (1986). Interactions of mothers with their infants who are mentally retarded, retarded with cerebral palsy, or nonretarded. American Journal of Mental Deficiency, 90(5) , 513-520.
- Harris, S. (1997). The effectiveness of early intervention for children with cerebral palsy and related motor disabilities. In Guralnick, M. (Ed.). The effectiveness of early intervention. Baltimore, MD: Paul H. Brookes, pp 327-347.
- Ketelaar, M., Vermeer, A. Helders, P.J.M. & Hart, H. (1998). Parent participation in programs for children with cerebral palsy: A review of research. Topics in Early Childhood Special Education, 18(2) , 108-117.
- Ketelaar, M., Vermeer, A., 't Hart, H., van-Petegem-van Beek, E. & Helders, P.J.M. (2001). Effects of a functional therapy programme on motor abilities of children with cerebral palsy. Physical Therapy, 81(9), 1534-1545.
- Mahoney, G. (1992). The Maternal Behavior Rating Scale-Revised. Available from the author, Family Child Learning Center, 143 Northwest Ave (Bldg A), Tallmadge, Ohio. 44278.
- Mahoney, G.J., Kim, J.M. & Lin, C.S. (in press). Parental responsiveness and children's pivotal behavior: The keys to intervention effectiveness. Infants and Young Children.
- Mahoney, G. & Perales, F. (2003). Using relationship-focused intervention to enhance the social-emotional functioning of young children with autism spectrum disorders. Topics in Early Childhood Special Education, 23(2) , 77-89.
- Mahoney, G. & Perales, F. (2005). A comparison of the impact of relationship-focused intervention on young children with Pervasive Developmental Disorders and other disabilities. Journal of Developmental and Behavioral Pediatrics, 26(2) , 77-85 .
- Mahoney, G., Robinson, C. & Fewell, R. (2001). The Effects of Early Motor Intervention on Children with Down Syndrome or Cerebral Palsy: A Field-Based Study. Developmental and Behavioral Pediatrics, 22 , 153-162.
- McCollum, J.A. & Hemmeter, M.L. (1997). Parent-child interaction intervention when children have disabilities. In M.J. Guralnick (Ed.), The effectiveness of early intervention (pp. 549-576). Baltimore: Brookes.
- Miller, L.J. & Roid, G.H. (1994). The T.I.M.E. Toddler Infant Motor Evaluation. Tucson, AZ, Therapy Skill Builders.
- Okimoto, A.M., Bundy, A. & Hanzlik, J. (2000). Playfulness of children with and without disability. American Journal of Occupational Therapy, 54(1) , 73-82.
- Palmer, F.B. (1997). Evaluation of developmental therapies in cerebral palsy . Mental Retardation and Developmental Disabilities Research Review, 3, 145-152.
- Palmer, F.B., Shapiro, P.K., Wachtel, R.C., Allen, M.C., Hiller, J.F., Harryman, S.E., Mosher, B.S., Meinert, C.L. & Caputo, A.J. (1988). The effects of physical therapy on diplegia. New England of Medicine, 318, 803-808.
- Rothberg, A.D., Goodman, M.J., Jacklin, L.A. & Cooper, P.A. (1991). 6-year follow-up of early physiotherapy intervention in very-low-birth-weight infants. Pediatrics, 88(3), 547-552.
- Sayers, L.K., Cowden, J.E. & Sherrill, C. (2002). Parents' perceptions of motor interventions for infants and toddlers with Down syndrome. Adapted Physical Activity Quarterly, 19(2), 199-219.
- Thelen, E. & Ulrich, B.D. ((1991). Hidden skills. Monograph of the Society for Research in Child Development, 56, 59-89, No. 223.
- Torres, C. & Buceta, J. (1998). Effect of parental intervention on motor development of Down syndrome infants between birth and two years. British Journal of Developmental Disabilities, 44(87), 94-101.
- Ulrich, D.A., Ulrich, B.D., Angulo-Kinzler, R.M. & Yun, J. (2001). Treadmill training of infants with Down syndrome: Evidence-based developmental outcomes . Pediatrics, 108(5), 42-48.
- Weindling, A.M., Hallam, P., Gregg, J., Klenka, H., Rosenbloom, L. & Hutton, J.L. (1996). A randomized controlled trial of early physiotherapy for high risk infants . Acta Paediatrica, 85(9) , 1107-1101.
- Wolery, M. (1983). Proportional change index: An alternative for comparing child change data. Exceptional Children, 50 , 167-170.

