Investigation of the articulatory patterns of young adults with Down syndrome using electropalatography
Tongue movements for speech in three adults with Down syndrome and one normal speaking control were investigatedusing electropalatography (EPG) and diadochokinetic rate (DDK)techniques. The subjects with Down syndrome all showedsubstantially larger areas of tongue-palate contact comparedwith the control subject for alveolar sounds /t, d, n, l/, anddifferences in fricative articulation. Undershoot (incompleteclosure) was a feature of velar articulations /k, g/ in the subjectswith Down syndrome. Longer closure duration, longer consonanttransition times within clusters and consistently slower DDKrates were also noted. Asymmetry and variabilitywere evident in two of the subjects with Down Syndrome.The results support the hypothesis that people with Downsyndrome have difficulties with coordinating the rapid tonguemovements necessary for clear speech with impaired tonguemotility and motor programming as well as phonological delay.Implications for treatment are discussed.
Hamilton, C. (1993) Investigation of the articulatory patterns of young adults with Down syndrome using electropalatography. Down Syndrome Research and Practice, 1(1), 15-28. doi:10.3104/reports.7
Introduction
Children and adults with Down syndrome have a higher incidence of speech (pronunciation) problems than any other group of people with severe learning difficulties (Schlanger and Gottsleben, 1957; Blanchard, 1964). In addition, their spontaneous speech and general intelligibility (speech clarity) lags behind their other language skills (Lenneberg, 1967; Ryan, 1975; Rondal, 1978). Intelligibility is a problem even in older children with Down syndrome who have more advanced syntax (Bray and Woolnough, 1988).
Although many reasons for the speech difficulties in people with Down syndrome have been proposed, it is far from clear which of many possible factors are actually involved. Intervention approaches have varied over the years, reflecting trends in both linguistic theory and in therapy. Even after periods of intervention, intelligibility often remains the greatest barrier to communication outside the family. Buckley and Sacks (1987) found that over half the adolescent girls and about 80 % of the adolescent boys in their survey were rated by their parents as unintelligible to strangers. Their intelligibility rating may have included issues of language skill difficulty (i.e. in forming sentences) but in my experience the major hindrance to effective communication in people with Down syndrome is poor speech clarity (pronunciation).
It seems likely that effective intervention has not been offered to this population because of a lack of objective assessment which in turn has led to unclear diagnoses of these speech problems.
This study aims to investigate the use of one objective measurement tool of speech articulation in an attempt to shed light on the complex nature of these speech difficulties.
Three main types of speech difficulty are possible in any person developing speech: dysarthria, dyspraxia and phonological delay/disorder. Dysarthria is due to muscle weakness and results in the slowing down or difficulty in coordination of the articulatory movements of the tongue and lips during speech. These "articulatory difficulties" can cause distortion of the speech sounds either by changing a sound slightly (e.g. slurring) or by changing a sound so it sounds like a different sound (e.g. "s" becomes "t").
Dyspraxia is thought to be due to a problem in the planning and execution of the sequence of movements needed for speech. It can result in inconsistent attempts at sounds (i.e. a word is said differently every time) and difficulty in sequencing consonant and vowel sounds in a word.
Phonological difficulties involve the delay or disordered development of the use of speech sounds and generally result in the simplification of words (e.g. "poo" for "spoon"). There are recognized patterns of development in the acquisition and use of sounds in children who are learning to talk. Phonological delays are said to occur when a developmental pattern is observed in a child's speech but the child is at an immature stage. Disorders are said to be when patterns not found in development are found.
From a review of the current and past literature, it seems that the speech difficulties of people with Down syndrome have been attributed by different researchers to: macroglossia (large tongue), hypotonia (muscle weakness), phonological delay/disorder (delayed development in the use of speech sounds), or a motor programming deficit (dyspraxia) (difficulty in planning and executing the sequence of movements needed to produce speech).
a) Macroglossia (Large tongue)
Both early and relatively recent literature attributes the speech difficulties in people with Down syndrome to the typically large or protruding tongue and small oral cavity found in most of them (Benda, 1949; Engler, 1949; Strazzula, 1953; Olbrisch, 1982). Many plastic surgeons who perform tongue reduction operations (partial glossectomy) on people with Down syndrome have claimed improvements in speech clarity as a result (Lemperle, 1980; Rozner, 1983; Wexler, 1986).
Others have questioned the effect of tongue size (Lenneberg, Nichols and Rosenberger, 1964; Rosenberg, 1982) including some plastic surgeons who have not found any significant effect on speech following tongue reduction operations (Margar-Bacal, Witzel and Munro, 1987; Klaiman, Witzel, Margar-Bacal and Munro, 1988 ; Parsons, Iacono and Rozner, 1987). In addition, some researchers, including Ardran and his colleagues (1972), the only researcher who used objective X-ray measures, have suggested that macroglossia in Down syndrome is an illusion due to the small size of the oral cavity; the need to mouth breathe because of a small nasopharynx (the upper part of the throat) and frequent upper respiratory tract infections; enlargement of the lingual tonsil in some cases; hypotonia of the tongue and lower lip; and forward position of the mandible with underdeveloped nasal and maxillary bones (the central part of the face) (Cohen and Winer, 1965; Krmpotic-Nemanic and Schulz, 1970; Ardran, Harker and Kemp, 1972; Purdy, Deitz and Harris, 1987; Yarom, Sherman, Sagher, Peled, Wexler and Gorodetsky, 1987 ).
A large tongue or a forward tongue position would not of itself guarantee a decrease in speech clarity - normal speech can be found with any anatomical deviation if the individual has learned to compensate for the defect (Bloomer, 1957).
b) Hypotonia (Muscle weakness)
There is strong evidence for hypotonia in Down syndrome muscles (McIntire and Dutch, 1964). Yarom et al. (1987) found evidence of degeneration of nerve endings and changes in the end plates of neuromuscular junctions in tongue tissue removed from people with Down syndrome in surgery. They suggest that this may be responsible for hypotonia in their tongues. Hypotonia in the tongue would lead to a "dysarthric" speech difficulty.
c) Phonological delay/disorder
Many studies over the past 15 years have focussed on the phonological development of people with Down syndrome (analysing their speech purely in terms of the acquisition and use of sounds) and have ignored or openly denied the possibility of articulatory difficulty (e.g. Dodd, 1984). Some have claimed speech development shows only delay (Stoel-Gammon, 1980; Rosenberg, 1982; Smith and Stoel-Gammon, 1983; Bleile and Schwarz, 1984; Rondal, 1988). Others feel there is disordered development (Dodd, 1975, 1976; Rosin, Swift, Bless and Vetter, 1988; Sommers, Patterson and Wildgen, 1988).
When errors are attributed to articulatory rather than phonological difficulties (e.g. Borghi, 1990), it is not clear how this decision was made. It seems that criteria are not based on objective measurement but on the theoretical background of the researcher and subjective auditory analysis (i.e. listening to the speech sample and then writing down phonetically what is thought to have been heard). That auditory assessments are far from accurate has already been shown (Oller and Eilers, 1975). This makes the need for objective measures of the speech of people with Down syndrome even more pressing.
It is important to note that even if the primary difficulty is one of articulatory control, compensatory strategies may give rise to whole sound changes which may then appear to be phonological simplifications (Crystal, 1981). For example, "skirt" could be produced "sirt" because of articulatory limitations or phonological simplification processes.
d) Motor programming deficits
Dodd (1976) proposed that people with Down syndrome have a central motor (muscle control) deficit resulting in problems with the planning and execution of fine motor (muscle) movements. Rosin, Swift, Bless and Vetter (1988) found that young adults with Down syndrome had more difficulty with speech production as demands for sequencing increased. They argue that difficulty with sequencing underlies both oral motor control and language, and suggest a pervasive processing problem in Down syndrome. Frith and Frith (1974) found evidence of impairment in the ability of children with Down syndrome to plan fine motor hand movements and this difficulty in establishing long-term motor programs for skilled movements has been related to cerebellar dysfunction in Down syndrome (Penrose 1963).
Difficulty in the planning and sequencing of sounds for speech would lead to a "dyspraxic" speech difficulty.
EPG data
The need for more objective data on the articulation patterns of people with Down syndrome is clear. The objective measurement tool chosen for this study was Electropalatography (EPG).
EPG is a technique developed over the past 30 years. It involves the use of an artificial palate made of acrylic, in which is embedded 62 silver electrodes arranged in 8 horizontal rows (see Figure 1.0).

Figure 1.0 Photograph of an EPG palate showing the silver electrodes and two wire clips to fit around the molar teeth
Each palate is tailor made for each subject and covers the hard palate so that any tongue contact with the electrodes on the palate during speech articulation can be recorded (see Figure 1.1). The electrode positions are determined by anatomical dimensions of the palate so that different palate sizes and shapes can be compared with reference to specific rows and electrode positions (Hardcastle, 1989).
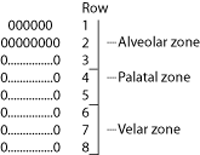
Figure 1.1. A computer generated display of tongue contacts (indicated by zeros) during the closure phase of /t/. This frame represents 10ms. Reference zones for the electrode positions and row numbers of electrodes are shown on the right.
From the EPG investigations already done, a range of normal patterns of tongue-palate contact for different sounds have been described (Hardcastle, 1984; Fletcher 1989; Hamlet, Bunnell and Struntz, 1986; Stone, Raphael and Shawker, in press). EPG has also been used to analyse the articulatory patterns of children and adults who have presented with a range of speech difficulties including dysarthria and dyspraxia (Hardcastle and Morgan, 1982; Hardcastle, Morgan Barry and Clark, 1985 and 198 7). The aim in the present study was to look for common patterns in the Down syndrome sample and compare them with existing EPG data of normal and disordered speech.
In order to attempt to differentiate between the different levels of breakdown proposed in the literature, a range of different monosyllabic and polysyllabic words/phrases were used and a test of Diadochokinetic rate (DDK) was completed. DDK testing involves counting the number of times certain sounds (e.g. p-p, p-t-k) can be repeated per minute. Difficulty in timing and sequencing of articulatory movements found in the polysyllabic words and DDK test would indicate difficulties at the motor programming level (dyspraxia).
Researchers have also shown interest in the processing skills of people with Down syndrome (their ability to take information from what they receive from their senses), claiming a deficit in auditory sequential processing compared with visual processing (O'Connor and Hermelin, 1965; Bilovsky and Share, 1965; Nakamura, 1965; Rohr and Burr, 1978; Rosin et al, 1988; Snart, O'Grady and Das, 1982). The use of visual systems, such as signing and reading, in teaching and facilitating speech and language learning in Down syndrome is widespread. Assuming that people with Down syndrome are able to convert letters and letter groupings to speech sounds (the "grapheme-phoneme" conversion route) (Ellis and Young, 1988), read words should be clearer than spontaneous output as information about the sequential order of each sound is given. Imitated words should not be as clear as read words if auditory processing deficits exist. My clinical experience supports this theory.
In this study, the same target words were elicited in three different conditions: picture naming (spontaneous recall), imitation (auditory input) and reading (visual input).
Methodology
Subjects
Three young adults with Down syndrome (Nikki, Michael and Paul) participated in this study with one non-disabled adult for comparison.
The young people with Down syndrome were selected on the basis of:
- having adequate comprehension to follow explanations of what was to be required of them and therefore be able to agree to take part.
- "typical" speech patterns for people with Down syndrome.
- differing levels of phonological development to allow analysis of fricatives, affricates, consonantal clusters as well as plosives.
- expressive language output of at least two word sentences to allow the use of phrases in the EPG target word lists.
The person recorded for comparison (Fiona) was a research speech therapist.
Speech, language and hearing tests were carried out on Nikki, Michael and Paul. These included: the TROG, which tests understanding of language and grammar; the LARSP, which is an analysis of expressive language (sentences) and PACS which is an analysis of phonology (speech sound acquisition and use). The results are shown below:
| Name | Age | Hearing levels | TROG | LARSP | PACS |
|---|---|---|---|---|---|
| Michael | 17 | High frequency loss | 5yrs | III 2-2.6yrs | IV 2.6-3yrs |
| Nikki | 17 | NAD | 6yrs | III/IV 2.6yrs | VI 3.6-4.6yrs |
| Paul | 20 | NAD | 4yrs | II 1.6-2yrs | IV 2.6-3yrs |
| TROG (Bishop, 1982); LARSP (Crystal, Fletcher and Garman, 1976); PACS (Grunwell, 1985). | |||||
Materials
- EPG palates were manufactured for each of the people in the study. In addition, practice palates (without electrodes) were made for Nikki, Michael and Paul. This was so that they could get used to wearing the palates before the EPG readings were taken.
- 54 target words were used to provide data for EPG analysis. The word list was taken from an EPG study by Hardcastle, Morgan Barry and Clark (1987) with the addition of 12 polysyllabic words/phrases (see Appendix).
- Black and white line drawings of all the target words were made on postcard size white card. Some use of colour was allowed when a colour adjective was required for the target response. No written words were visible on the pictures. For the reading condition, target words were hand written onto the card in black ink with lower case letters.
- The EPG hardware and software used in this study was developed by researchers at Reading University and IBM Scientific Centre, Winchester ( Hardcastle, Jones, Knight, Trudgeon and Calder, 1989 ).
Procedures
- Nikki, Michael and Paul wore their practice palates for an hour per day in the fortnight prior to their EPG analysis. In addition, practice palates were worn for the 2 hours immediately before the actual data collection. Fiona was an experienced palate user and so did not require these adjustment periods (Hamlet and Stone 1978).
- Nikki, Michael and Paul received four visits from the researcher to ensure recognition of the picture items and written words and to ensure familiarity with the procedures to be adopted in the data collection.
- The target words were presented in three different conditions in this order: (1) as spoken words for imitation, (2) as pictures, (3) as written words. The items were placed in random order within the three conditions. In the third condition, only those words that were able to be read (as assessed on the pre-EPG visits) were shown. One of the young people with Down syndrome was unable to read, another could only read 34 out of the 54 words, the third could read all the words. EPG patterns for all these test items were stored on disc for analysis.
- A DDK rate measurement was taken for Nikki, Michael and Paul using the time-by-count technique (Fletcher 1972).
Results
Nikki, Michael and Paul's EPG patterns for different sounds were studied and compared with those of Fiona and the normal patterns described by Hardcastle (1984) and Hardcastle et al. (1987). The Reading University EPG software includes the facility to list the number of tongue-palate contacts across three zones of the palate: alveolar, palatal and velar (please see Figure 1.0).
These contact totals were taken at the point of maximum tongue-palate contact during each sound. The point of maximum contact is a measure that has been used widely by other researchers (Hiki and Itoh, 1986; Hardcastle et al, 1989; Fletcher, 1989) and although it is an arbitrary point, it provides a useful and easily identifiable landmark in the articulation of the sound, for comparison across subjects.
A summary of the tongue-palate contact patterns for each group of sounds analysed is given:
Alveolar stops (/t,d,n/)
The most striking finding was the amount of palatal contact for these sounds in Nikki, Michael and Paul. All showed at least one row of contacts in the palatal zone in addition to full alveolar zone contact. Compare this with Fiona who only ever showed contact with the anterior two alveolar rows when articulating t, d or n sounds (see Figure 1.2 and Table 1). The actual pattern of tongue-palate contacts, traced onto a two dimensional representation of each subject's palate is illustrated in Figure 1.2. The pattern shown is that occurring during the point of maximum tongue-palate contact for /d/ in "dart". The actual EPG printout of the source frame is also shown. The use of more palatal and velar zone contacts is clearly visible in Nikki, Michael and Paul's EPG patterns.

Figure 1.2. Maximum contact patterns for /d/ in "dart"
| Name | Alveolar | Palatal | Velar |
|---|---|---|---|
| FIONA | 13.62 | 9.33 | 7.04 |
| NIKKI | 14.00 | 20.37 | 10.78 |
| MICHAEL | 13.28 | 23.35 | 13.83 |
| PAUL | 13.29 | 17.65 | 8.43 |
Velar stops (/k,g/)
Nikki, Michael and Paul again showed differences from Fiona, with inadequate and incomplete tongue-palate contact (undershoot) being the most noticeable feature. However, Michael used almost total contact with the palate for /ng/. (See Figures 1.3 and 1.4 and Table 2).
Figure 1.3. Maximum contact patterns for /k/ in "keys"
Figure 1.4. Maximum contact patterns for /ng/ in "singing"
| Name | Alveolar | Palatal | Velar |
|---|---|---|---|
| FIONA | 0 | 3.14 | 17.22 |
| NIKKI | 0 | 0 | 14.38 |
| MICHAEL | 0.21 | 0.47 | 12.04 |
| PAUL | 0.22 | 3.58 | 11.10 |
Laterals /l/
Again more palatal and velar contacts were evident in the young adults with Down syndrome compared with Fiona. Michael also showed less alveolar contact with the main constriction being at rows 3/4. His /l/ articulations showed a great deal of variability (see Figure 1.5).

Figure 1.5. Maximum contact patterns for /l/ in"leaf"
Asymmetry was a feature of /s/ and /sh/ in Paul and Michael, with increased palatal zone contacts for /s/ and a similar pattern for /sh/ (they were difficult to distinguish auditorily as well). In Michael the constriction was made at rows 3/4 and too much tongue-palate contact (overshoot) was a frequent feature. (See Figures 1.6 and 1.7).
Figure 1.6. Maximum contact patterns for /s/ in "seed" Fricatives (/s,sh/)
Figure 1.7. Maximum contact patterns for /sh/ in "shoe"
Overlapping articulations
In consonant clusters and syllable boundaries where consonant coarticulation (overlapping articulation) was expected to be found, only Fiona showed consistent patterns. Nikki, who had the clearest speech showed no overlapping articulations at all. For example "tickling" was produced as "tickeling" by Nikki and Michael (see Figure 1.8). Where faster transitions were seen, it was often at the "expense" of one of the sounds, i.e. assimilation occurred (see Michael's /sk/ in "skirt", Figure 1.9).
Figure 1.9. EPG patterns for /sk/ in "skirt"
Polysyllabic words
In Michael and Paul, these often showed such a degree of assimilation and simplification that the EPG patterns were not easily analysable. Nikki showed no coarticulatory patterns even in longer phrases and also tended to simplify by omitting sounds. She took longer to say the phrases than the control subject and showed longer closure durations and approaches to each sound.
Durations
Some apparent differences in the duration of initial plosives was also evident in the young adults with Down syndrome. Nikki in particular showed very long durations (see Table 3). Paul showed a great deal of variability in closure durations.
| Name | Average duration (number of 10ms frames) across conditions |
|---|---|
| FIONA | 9.17 frames |
| NIKKI | 30.75 frames |
| MICHAEL | 13.22 frames |
| PAUL | 38.00 frames |
DDK rates
These were significantly slower than the norms given. The experimental subjects found it extremely difficult to maintain a steady repetition of these sounds and had particular difficulty with the /p-t-k/ sequence (see Table 4).
| Name | /p/ | /t/ | /k/ | /f/ | /l/ | /pt/ | /pk/ | /tk/ | /ptk/ |
|---|---|---|---|---|---|---|---|---|---|
| NIKKI | 9.0 | 7.3 | 10.5 | 7.0 | 6.0 | 13.5 | 16.0 | 16.0 | 27.0 |
| MICHAEL | 9.2 | 7.3 | 9.2 | 8.9 | 6.5 | 9.0 | 8.5 | 20.0 | 19.0 |
| PAUL | 8.0 | 9.0 | 7.0 | 8.3 | 9.0 | 9.1 | 14.0 | 13.0 | * |
| "Norms" | 4.8 | 4.9 | 5.5 | 5.5 | 5.2 | 7.3 | 7.9 | 7.8 | 10.3 |
| KEY: 1. The scores represent the time in seconds required for 20 repetitions of single syllables, 15 repetitions of bisyllables (e.g. /pt/) 10 repetitions of /ptk/. 2. Each sound was produced as a CV (consonant-vowel) utterance - the schwa vowel (as in the) following the consonant. 3. Norms given are for 6 year olds (Fletcher 1972) - see text for explanation. * Paul was unable to say this sequence of sounds even after repeated prompting. Michael's /tk/ was actually /t-t/ for more than half of his attempt. | |||||||||
Differences between conditions
The EPG patterns for the different sounds did not differ across the three conditions (imitation, reading and spontaneous speech) for any of the subjects in the study.
Individual differences
Nikki had the clearest speech. She also spoke very slowly - this could have been a compensatory strategy, but it is interesting to note that she also had very slow approach phases to her sounds: compare her approach to closure for /n/ in "knot" with that of the others (see Figure 2.0). It is unlikely that this is a learned strategy - it may be indicative of difficulty in executing rapid tongue movements or indicate some underlying dysfluency.

Michael often released his closures atypically, in anterior to posterior direction (tongue tip/blade first). Michael showed the largest areas of contact of all the subjects. He also appeared to have the largest tongue (from observation) and the shallowest palate. In addition, he had the most difficulty in adjusting to the EPG palate. These factors may all be related to the EPG patterns found in his sample.
Paul's speech was the least intelligible. He had a tendency to place the middle of his tongue up to the hard/soft palate areas during speech (particularly strange as he had a very steep, high palate). (See Figure 2.1)
Figure 2.1. Paul's EPG printout for "leg" showing the persistent line of velar contacts (see text for explanation)
Phonological processes
Developmental phonological patterns were also found in the data: final consonant deletion (e.g. "see" for "seed"), consonant harmony (e.g. "gog" for "dog"), fronting ("fis" for "fish"), stopping of fricatives ("dot" for "dolls"), cluster reduction (e.g. "bak" for "black"). However these can not account for the articulatory differences described above.
Summary of results
In brief, the young adults with Down syndrome shared the following differences from Fiona (whose EPG patterns were consistent with the normal data (Hardcastle op.cit.)):
- More palatal zone contact
- Undershoot with velar articulations
- Longer closure durations
- Difficulty with rapid tongue movements both in longer words and in the DDK tests.
- Limited use of consonantal coarticulation
- Phonological processes reducing the number of sound contrasts used.
In Michael and Paul, asymmetry and variability were features of fricative articulation.
Discussion
Various theories have been proposed regarding the level of impairment in the speech production processes of people with Down syndrome.
The results in this study lend some support to the theory of an articulatory level of impairment which could result from hypotonia.
The increased tongue-palate contact patterns found in this study were also found in dysarthric children by Hardcastle (1987).
Movement of the tongue body up and back to the velar area for /k,g/ sounds also appeared to be slower in Nikki, Michael and Paul compared to Fiona. /k,g/ sounds were produced as fricatives (as in the Scottish "loch") or omitted. This "undershoot" is also a feature of dysarthric speech (Hardcastle, 1985).
Overshoot for fricatives (too much tongue-palate contact) resulting in complete closure, evident in Michael's speech, was also found in Hardcastle's 1985 sample.
The absence of any adequate auditory or articulatory difference between /s/ and /sh/ which is common in dysarthria was also evident in Michael and Paul.
The absence of coarticulatory patterns in consonantal clusters is another feature of dysarthric speech (Hardcastle, 1989) and was also found in Nikki, Michael and Paul. Presumably the difficulty of moving both the tip/blade (front) and the body (back) of the tongue to different places on the palate at the same time requires more accurate control than is possible in hypotonic tongues (Butcher, 1989).
It is also possible that some of the immature phonological patterns that were found in Nikki, Michael and Paul's speech may have been a by-product of limitations in tongue movement rather than evidence of delayed phonological maturation.
In all of the young adults with Down syndrome, there were some alveolar sounds where the tongue tip actually protruded forward from the incisor teeth during their articulation. For these sounds, the tongue tip was not used at all in articulation. As the somewhat larger area immediately posterior to the tip (the tongue "blade") was presumably used instead, this alone might account for the increased areas of palatal contact. This may lend credence to the macroglossia argument - that the larger size and more forward tongue position are the reasons for poor speech clarity in people with Down syndrome (Fucci and Petrosino, 1981).
However, one could also question why the tongue tip was not used during speech - in my clinical experience of other children with speech difficulties, a tongue tip protrusion pattern at rest does not usually affect articulation of alveolar plosives - /t,d,n/ (i.e. the tongue tip is still used in articulation). It must also be noted that for the alveolar sounds where the tongue tip was inside the mouth, the pattern of more electrode contact was still evident. This suggests some difficulty in controlling the tongue tip itself. This finding would also support the hypotonia argument.
Difficulties in motor programming for speech articulation would lead to dyspraxic type abnormalities in the timing and sequencing of movements. These are also evident in the data collected.
Dyspraxic speakers show long closure durations (Hardcastle, 1985) - also found in the young adults with Down syndrome in this study. In addition, Hardcastle noted slow approach and release phases for closures in his dyspraxic subjects - a feature of Nikki's EPG data also.
Abnormally long transitions between different elements in consonant clusters, another feature of dyspraxic speech, is also found in Nikki's and Michael's data.
The great difficulty experienced by Nikki, Michael and Paul in rapidly repeating polysyllabic Consonant-Vowel sequences in the DDK test is also indicative of motor sequencing (dyspraxic) problems (Henry 1990). The subjects' erratic and arrhythmic production of these sequences is also typical of dyspraxic difficulty (Henry 1990).
Asymmetry and variability, particularly noted in the /s/ and /sh/ articulations of Michael and Paul are also features of dyspraxic speech (Johns and Darley, 1970; Hardcastle, 1989 and personal communication).
The three different conditions in this study did not appreciably affect the performance of any of the subjects. This may have been due to practice effects (the same words were used in all conditions and had been practised beforehand). In addition, specific training in using the grapheme-phoneme route for word recognition may have been necessary before beneficial effects would be seen.
From the results discussed above, it seems that there is evidence in these young adults with Down syndrome, for breakdown both in the ability to move the tongue and lips in order to articulate speech sounds accurately and in the ability to select, plan and sequence the sounds needed. These are in addition to phonological difficulties. All of these factors would contribute to making the speech of people with Down syndrome unintelligible.
There are a number of clinical implications of these findings.
In the past there has been a tendency to focus on intervention to improve phonological rather than articulatory skills. It seems clear that tongue motor coordination must be an area for work as well as encouraging phonological development. There is a need for further studies evaluating the effects of any possible treatment methods (e.g. Proprioceptive Neuromuscular Facilitation (Langley and Darvill, 1979). Perhaps EPG could be used to measure any articulatory changes.
The practice of removing part of the tongue, widely heralded as a technique to improve cosmetic appearance and speech is certainly contra-indicated by these findings. As it is clear from the results of this study that the speech difficulties of people with Down syndrome can not be attributed purely to macroglossia, removing weak tongue muscle tissue would seem at the very least an ineffective treatment and certainly inadvisable.
The use of EPG in treatment has been documented (Morgan Barry, 1989) and it may be an effective way of providing visual feedback for this client group. Certainly the experimental subjects showed considerable interest and understanding of their tongue-palate patterns shown on the visual display.
Further research is needed into what happens to articulation and phonology in spontaneous speech and in longer utterances. There is evidence for increased error rate in spontaneous speech in people with Down syndrome (Sommer, Patterson and Wildgen, 1988).
Conclusions
In this study, the young adults with Down syndrome showed evidence of impaired muscular control of the tongue resulting in slow movements, difficulty in tongue tip control and coarticulation. Difficulty in planning sequences of articulatory actions was also found, resulting in long closure durations, long transitions between consonants within clusters, erratic DDK output, asymmetry and variability in some articulations.
It is clear that the speech difficulties experienced by people with Down syndrome are complex. This study suggests that they are due to impairments at virtually every level of the speech production process - selecting the sounds (phonological), planning their sequence (motor programming) and carrying out the movements of the tongue and lips (articulatory). Assessment and treatment must therefore reflect this complexity and clinicians must be prepared not only to work at these different levels but also to evaluate which treatment approaches are effective for the different impairments. By this means, it is hoped that people with Down syndrome will be able to communicate more intelligibly and consequently enjoy more opportunities for an independent life.
Appendix
Target words used for EPG analysis
Glossary
- Alveolar: A sound which is made by tongue contact on the alveolar ridge.
- Articulation: The movements of the tongue and lips in relation to the palate that produce speech sounds.
- Closure: Contact between the tongue and palate which impedes the airflow (shown as a complete line of EPG zeroes in stop articulations).
- Coarticulation: The overlapping of adjacent articulations.
- Consonant clusters: Sounds where two consonants articulations are adjacent e.g. cl, st, sk.
- Consonant Harmony: The phonological rule that makes all consonant sounds in a word the same e.g. "gog" for "dog".
- Dyspraxia: A disorder of speech that is said to result in difficulties in the planning, selection and sequencing of sounds.
- Dysarthria: A disorder of speech as a result of impaired muscular control.
- DDK: Diadochokinetic rate - a measure of speed of articulatory movements. It involves rapid repetition of consonant-vowel sequences.
- EPG frame: Each 10ms tongue-contact pattern is called a frame.
- Fronting: The phonological rule that substitutes more anterior articulations for posterior ones e.g. "tar" for "car".
- Fricative: Narrowing of the distance between two articulators so that the airstream is partially obstructed and a turbulent airflow is produced, as in /s/.
- Grapheme-phoneme route: The hypothesised conversion of letters and letter groupings to sounds which occurs when reading unfamiliar words.
- Hypotonia: Low muscle tone leading to weak muscle function.
- Language: The understanding and expression of words and sentences.
- LARSP: Language Assessment Remediation Screening Procedure.
- Lateral: An articulation in which the airstream flows over the sides of the tongue, as in /l/.
- Macroglossia: A condition where the tongue is abnormally large.
- Maximum contacts: The point at which the tongue has the most contact with the palate in any sound.
- NAD: No abnormality detected.
- Overshoot: Increased tongue contact caused by difficulty in controlling the tongue resulting for example in complete closure for a fricative articulation.
- PACS: Phonological Assessment of Child Speech.
- Palate: The roof of the mouth from the alveolar ridge to the margin of the soft palate (velum).
- Palatal: A sound articulated by tongue contact with the hard palate (posterior to the alveolar ridge).
- Phonology: The description of systems of sounds that give contrastive meanings to words.
- Phonetic transcription: Detailed representation of a sound.
- Polysyllables: An utterance containing more than two syllables.
- Schwa vowel: The vowel in "the" or "a".
- Speech: The production of sounds that make up words.
- Stop: Complete closure of two articulators. Examples of stops are : p, t, d, k, n.
- TROG: Test for Reception of Grammar.
- Undershoot: This is when the tongue fails to make adequate contact with the palate for either fricatives or stops. In stops this is more evident and results in incomplete closure.
- Velar: An articulation involving the back of the tongue and the velum, or soft palate. Velar sounds include /k, g, ng/.
Acknowledgement
This research was supported by a grant from the College of Speech and Language Therapists. The author wishes to thank Professor W J Hardcastle and Fiona Gibbon at the Department of Linguistic Science, Reading University, for their help and advice in carrying out this study.
References
- Ardran, G. M.,Harker, P. and Kemp, K. H. (1972) Tongue size in Down Syndrome. Journal of Mental Deficiency Research, 16 (3), 160-166.
- Benda, C. E. (1949) Mongolism and Cretinism. New York: Grune and Stratton.
- Bilovsky, D. and Share, J. (1965) The ITPA and Down syndrome: an exploratory study. American Journal of Mental Deficiency, 70, 78-82.
- Bishop, D. V. M. (1982) Test for Reception of Grammar (TROG). Manchester: Chapel Press.
- Blanchard, I. (1964) Speech pattern and etiology in mental retardation. American Journal Mental Deficiency, 68, 612-617.
- Bleile, K. and Schwarz, I. (1984) Three perspectives on the speech of children with Down Syndrome. Journal of Communication Disorders, 17, 87-97.
- Bloomer, H. H. (1957) Speech defects associated with dental abnormalities and malocclusions. In L. E. Travis (Ed) Handbook of Speech Pathology, 608-652. New York: Appleton - Century.
- Borghi, R. W. (1990) Consonant phoneme, and distinctive feature error patterns in speech. In D. C. van Dyke, D. J. Lang, F. Heide, S. van Duyne & M. J. Soucek (Eds) Clinical Perspectives in the Management of Down Syndrome. New York: Springer-Verlag.
- Bray, M. and Woolnough, L. (1988) The language skills of children with Down Syndrome aged 12-16 years. Clinical Language Teaching and Therapy, 4 (3), 311-324.
- Buckley, S. and Sacks, B. (1987) The Adolescent with Down Syndrome - Life for the teenager and for the family. Portsmouth Down Syndrome Trust: Portsmouth.
- Butcher, A. (1989) Measuring coarticulation and variabilty in tongue contact patterns. Clinical Linguistics and Phonetics, 3 (1), 39-47.
- Cohen, M. M. and Winer, R. A. (1965) Dental and facial characteristics in Down Syndrome. Journal of Dental Research, 44 (supplement), 197-298.
- Crystal, D. (1981) Clinical Linguistics. Disorders of Human Communication vol. 3. Wien, New York: Springer-Verlag.
- Crystal, D., Fletcher, P. and Garman, M. (1976) The grammatical analysis of language disability: a procedure for assessment and remediation. Studies in Language Disability and Remediation 1. London: Arnold.
- Dodd, B. (1975) Recognition and reproduction of words by Down syndrome and non-Down syndrome retarded children. American Journal of Mental Deficiency, 80 (3), 306-311.
- Dodd, B. (1976) A comparison of the phonological systems of mental age matched normal, severely subnormal and Down Syndrome children. British Journal of Communication Disorders, 11, 27-42.
- Dodd, B. and Leahy, J. (1984) Down Syndrome and tongue size (letter). The Medical Journal of Australia, June 9th, 748.
- Ellis, A. and Young, A. (1988) Human Cognitive Psychology. Hove and London: Lawrence Erlbaum Associates.
- Engler, M. (1949) Mongolism. Baltimore: Williams and Wilkins.
- Fletcher, S.G. (1972) Time-by-count measurement of Diadochokinetic rate. Journal of Speech and Hearing Research, 15, 763-770.
- Fletcher, S. G. (1989) Palatometric specification of stop, affricate and sibilant sounds. Journal of Speech and Hearing Research, 32, 736-748.
- Frith, U. and Frith, C. D. (1974) Specific motor disabilities in Down Syndrome. Journal Child Psychology and Psychiatry, 15, 293-301.
- Fucci, D. and Petrosino, L. (1981) The human tongue: normal structure and function and associated pathologies. In N. J. Lass (Ed) Speech and Language Advance in Basic Research and Practice, volume 6. London: Academic Press.
- Grunwell, P. (1985) Phonological Assessment of Child Speech (PACS). Windsor: NFER Nelson.
- Hamlet, S. L., Bunnell, H. T., and Struntz, B. (1986) Articulatory asymmetries. Journal of Acoustic Society of America, 79,(4), 1164-1169.
- Hamlet, S. L. and Stone, M. (1978) Compensatory alveolar consonant production induced by wearing a dental prosthesis. Journal of Phonetics, 6, 227-248.
- Hardcastle, W.J. (1984) New methods of profiling lingual-palatal contact patterns with electropalatography. Phonetics Laboratory University of Reading Work in Progress, 4, 1-40.
- Hardcastle,W.J. and Morgan,R.A. (1982) Experimental investigation of articulatory disorders in children. British Journal of Communication Disorders, 17,47-65.
- Hardcastle,W.J., Jones, W., Knight, C., Trudgeon, A. and Calder, A. (1989) New developments in electropalatography: a state-of-the-art report. Clinical Linguistics and Phonetics, 3 (1), 1-38.
- Hardcastle,W.J., Morgan Barry,R.A. and Clark,C.J. (1985) Articulatory and voicing characteristics of adult dysarthric and verbal dyspraxic speakers: an instrumental study. British Journal of Disorders of Communication, 20, 249-270.
- Hardcastle,W.J., Morgan Barry, R. A. and Clark, C. J. (1987) An instrumental phonetic study of lingual activity in articulation-disordered children. Journal of Speech and Hearing Research, 30 (June), 171-184.
- Henry, C. E. (1990) The development of oral diadochokinesia and nonlinguistic rhythmic skills in normal and speech disordered young children. Clinical Linguistics and Phonetics, 4, (2), 121-137.
- Hiki, S. and Itoh, H. (1986) Influence of palate shape on lingual articulation. Speech Communication, 5, 141-158. Johns, D. F. and Darley, F. L. (1970) Phonetic variability in apraxia of speech. Journal of Speech and Hearing Research, 13, 556-583.
- Klaiman, P., Witzel, M. A., Margar-Bacal, F. and Munro, I. R. (1988) Changes in aesthetic appearance and intelligibility of speech after partial glossectomy in patients with Down Syndrome. Plastic and Reconstructive Surgery, September, 403-408.
- Krmpotic-Nemanic, J. and Schulz, J. (1970) Low set ears and small oral cavity with relative macroglossia in Down Syndrome. Chicago Medical School Quarterly, 30, (1), 41-45.
- Langley, J. and Darvill, G. (1979) Procedures for facilitating improvements in swallow, mastication, speech and facial expression where these have been impaired by central or peripheral nerve damage. London: NHCSS.
- Lemperle, G. and Radu, D. (1980) Facial plastic surgery in children with Down Syndrome. Plastic and Reconstructive Surgery, 66, 337-342.
- Lenneberg, E. H. (1967) Biological Foundations of Language. New York: John Wiley and Sons.
- Lenneberg, E. H., Nichols, I. R. and Rosenberger, E. F. (1964) Primitive stages of language development in mongolism. In D. M. Rioch and E. A. Weinstein (Eds) Disorders of Communication. Association for research in nervous and mental disease, vol. XLII. Baltimore: The Williams and Wilkins Company.
- Margar-Bacal, F., Witzel, M. A. and Munro, I. R. (1987) Speech intelligibility after partial glossectomy in children with Down Syndrome. Plastic and Reconstructive Surgery, 79, (1), 44-47.
- McIntire, M. S. and Dutch, S. J. (1964) Mongolism and generalized hypotonia. American Journal of Mental Deficiency, 68, 669-670.
- Morgan Barry, R. (1989) EPG from square one: an overview of electropalatography as an aid to therapy. Clinical Linguistics and Phonetics, 3 (1), 81-91.
- Nakamura, H. (1965) An inquiry into systematic differences in the abilities of institutionalized adult mongoloids. American Journal of Mental Deficiency, 69, 661-665.
- O'Connor, N. and Hermelin, B. (1965) Sensory dominance. Archives General Psychiatry, 14, 99-103.
- Olbrisch, R. R. (1982) Plastic surgical management of children with Down Syndrome: indications and results. British Journal of Plastic Surgery, 35, 195-200.
- Oller, D. K. and Eilers, R. E. (1975) Phonetic expectation and transcription validity. Phonetica, 31, 288-304.
- Parsons, C. L., Iacono, T. A. and Rozner, L. (1987) Effect of tongue reduction on articulation in children with Down Syndrome. American Journal of Mental Deficiency, 91, 328-332.
- Penrose, L. S. (1963 The Biology of Mental Defect. (2nd Edition). London: Sidgwick and Jackson.
- Purdy, A. H., Deitz, J. C. and Harris, S. R. (1987) Efficacy of two treatment approaches to reduce tongue protrusion of children with Down Syndrome. Developmental Medicine and Child Neurology, 29, 469-476.
- Rohr, A. and Burr, D. B. (1978) Etiological differences in patterns of psycholinguistic development of children of IQ 30 to 60. American Journal of Mental Deficiency, 82, 549-553.
- Rondal, J. A. (1978) Maternal speech to normal and Down Syndrome children matched for mean length of utterance. In E. Meyers (Ed) Quality of Life in Severely and Profoundly Mentally Retarded People. Washington DC: Research Foundations for Improvement, American Association on Mental Deficiency.
- Rondal, J. A. (1988) Down Syndrome. In D. Bishop and K. Mogford Language development in exceptional circumstances. London: Churchill Livingstone.
- Rosenberg, S. (1982) The language of the mentally retarded: development, processes and intervention. In S. Rosenberg (Ed) Handbook of Applied Psycholinguitics, Major Thrusts of Reasearch and Theory. New Jersey: Lawrence Erlbaum Associates.
- Rosin, M. M., Swift, E., Bless, D. and Vetter, D. K. (1988) Communication profiles of adolescents with Down Syndrome. Journal of Childhood Communication Disorders, 12 (1), 49-64.
- Rozner, L. (1983) Facial plastic surgery for Down Syndrome. Lancet, June 11th, 1320-1323.
- Ryan, J. (1975) Mental subnormality and language development. In E. H. Lenneberg and E. Lenneberg (Eds) Foundations of Language Development: a multidisciplinary approach, vol. 2. London: Academic Press.
- Schlanger, B. and Gottsleben, R. H. (1957) Analysis of speech defects among the institutionalized mentally retarded. Journal of Speech and Hearing Disorders, 22, 98-103.
- Smith, B. L. and Stoel-Gammon, C. (1983) A longitudinal study of the devlopment of stop consonant production in normal and Down Syndrome children. Journal of Speech and Hearing Disorders, 48, 114-118.
- Snart, F., O'Grady, M., and Das, J. P. (1982) Cognitive processing by subgroups of moderately mentally retarded children. American Journal of Mental Deficiency, 86 (5), 465-472.
- Sommers, R. K., Patterson, J. P. and Wildgen, P. L. (1988) Phonology of Down Syndrome speakers, ages 13-22. Journal of Childhood Communication Disorders, 12 (1), 65-91.
- Stoel-Gammon, C. (1980) Phonological analysis of four Down Syndrome children. Applied Psycholinguistics, 1, 31-48.
- Stone, M., Raphael, L. J. and Shawker, T. H. (in press) Cross-sectional tongue shape and lingua-palatal contact patterns in [s],[sh] and [l]. Journal of Speech and Hearing Research.
- Strazzulla, M. (1953) Speech problems of the mongoloid child. Quarterly Review of Paediatrics, 8, 268-272.
- Wexler,M.R., Peled,I.J., Rand,Y., Mintzker,Y. and Feuerstein,R. (1986) Rehabilitation of the face in patients with Down Syndrome. Plastic and Reconstructive Surgery, 77 (3), 383-391.
- Yarom, R., Sherman, Y., Sagher, U., Peled, I. J., Wexler, M. R. and Gorodetsky, R. (1987) Elevated concentrations of elements and abnormalities of neuromuscular junctions in tongue muscles of Down Syndrome. Journal of the Neurological Sciences, 79, 315-326.

