Simultaneous treatment of grammatical and speech-comprehensibility deficits in children with Down syndrome
Children with Down syndrome often display speech-comprehensibility and grammatical deficits beyond what would be predicted based upon general mental age. Historically, speech-comprehensibility has often been treated using traditional articulation therapy and oral-motor training so there may be little or no coordination of grammatical and speech-comprehensibility treatment. The purpose of this paper is to provide the rationale for and preliminary evidence in support of integrating speech and grammatical intervention using a type of recast treatment in six children with Down syndrome. Speech-comprehensibility and MLU growth in generalisation sessions occurred in 4/6 and 5/6 participants, respectively. Using multiple baseline design logic, two of these participants showed evidence of treatment effects on speech-comprehensibility and two in MLU in generalisation sessions, respectively. The study constitutes a conservative test of the intervention effects for reasons that are discussed. The theoretical and applied significance of these findings are discussed.
Camarata, S, Yoder, P, and Camarata, M. (2006) Simultaneous treatment of grammatical and speech-comprehensibility deficits in children with Down syndrome. Down Syndrome Research and Practice, 11(1), 9-17. doi:10.3104/reports.314
Children with Down syndrome (Trisomy 21) often display a number of developmental delays in physical, social, and mental development (Miller & Leddy, 1999). In particular, preschoolers with Down syndrome tend to have deficits in productive syntax and speech that ultimately impact the speech-comprehensibility which is often below that expected for mental age, comprehension level, and even vocabulary level (Miller, 1999; Miller & Leddy, 1999). In this paper, we define speech-comprehensibility as understandable spoken language. We use this term rather than "intelligibility" because the latter term is applied to analyses in which the intended message is known (Kent, Miolo & Bloedel, 1994; Kent et al. 1989). During uncontrolled conversation, the most frequent language use context of young children with Down syndrome, the intended message is often, at least partly, unknown. Therefore, examining the extent to which an unfamiliar listener can understand what the child says (i.e., speech-comprehensibility) is a socially important outcome that can be derived from a socially important measurement context. Many believe that the speech-comprehensibility problems of children with Down syndrome are due largely to motor constraints (Miller & Leddy, 1999) and unique vocal tract structures (Leddy, 1999) and children with Down syndrome are routinely enrolled in speech therapy with the goal of improving speech accuracy, and ultimately, speech-comprehensibility.
Speech accuracy is the extent to which the child accurately produces the speech sounds in the words he or she uses as compared with the adult version of the words. For example, a child saying "ba wo" for "ball roll" may be comprehensible in that the adult understood the meaning of the child's production, but the speech accuracy of the production if measured in percent consonants correct (PCC) would be 33% (b correct and the final "l" in ball and roll incorrect and "r" incorrect in "roll"). This example illustrates that assessments of speech accuracy will not necessarily tell us about a child's speech-comprehensibility. Thus, it is not surprising that studies of children with speech problems indicate that the measures of speech accuracy (e.g., percentage consonants correct) explain only an average of 16% of the percentage word attempts for which words are transcribed, even though both measures are derived from the same speech samples (Shriberg & Kwiatkowski, 1982; Shriberg, Kwiatkowski, Best, Hengst & Terselic-Weber, 1986). It is reasonable to consider speech-comprehensibility as a socially important outcome. The distinction between speech accuracy and speech-comprehensibility is used in the adult disability literature (e.g., dysarthria secondary to stroke, Hanson, Yorkston & Beukelman, 2004) and appears to be a useful distinction in children with Down syndrome as well.
Similarly, it is well known that grammatical acquisition is often problematic in Down syndrome (e.g., see Chapman et al., 2000; Miller, 1999) and children with Down syndrome typically receive grammatical intervention as well. For example, there are a number of procedures available to improve language skills in children with disabilities that focus on the use of naturalistic routines as a context for learning. For example, the Child Talk model emphasises language acquisition as an outcome of a large, accumulating database of language experienced or use in communicative contexts (Chapman, Streim, Crais, Salmon, Negri & Strand, 1992). Citing the Child Talk model, Chapman (1999) asserted that using routine event contexts to support communicative learning is expected to be especially effective in facilitating acquisition and generalisation. Verbal routines are familiar, predictable turn-taking conversations or games in which both members of the dyad have spoken turns (Yoder, Spruytenburg, Edwards & Davies, 1995). Routines may aid children in processing linguistic input because the repetitive nature and predictability of the exchange increases their comprehension of adult utterances and their role in the interaction (Shatz, 1983). Empirically, children with developmental delays have been found to talk more frequently and with more diverse vocabulary (Yoder & Davies, 1992a) and are more intelligible to adults (Yoder & Davies, 1992b) in verbal routines than in nonroutine interactions. Using frequency, diverse, and comprehensible platform utterances provide more opportunities for clinicians to use another intervention technique: recasts (Camarata, Nelson & Camarata, 1996; Camarata & Nelson, in press).
There are at least two primary classes of recasts: grammatical (adult utterances that add grammatical information to the child's platform utterance) and speech (adult utterances that add only phonemic information to the child's platform utterance; see Camarata, 1993, 1996). These adult utterances are used immediately after the child speaks. They are thought to be effective because of the temporal proximity and semantic overlap with the preceding child's utterance (i.e., the platform utterance). These attributes are hypothesised to aid the child in comparing his platform utterance with the recast thus making the new linguistic information salient (Nelson, 1989). When taking place in the context of an emotionally positive interaction about an event of interest to the child that includes an aspect of language the child is ready to acquire, the probability of acquisition is much heightened (Nelson, 1989). Finally, there is information suggesting that frequent recasts are necessary for children with language disorders to increase grammatical skills (Proctor-Williams, Fey & Frome-Loeb, 2001). A combination of recasts and verbal routines may increase the frequency that children with Down syndrome process linguistic input designed to provide them with grammatical and speech information needed to enhance their productive grammar and speech-comprehensibility.
Interestingly, speech-comprehensibility and grammatical skills are often viewed as distinct, almost orthogonal areas for intervention. Children with Down syndrome will often have a series of speech production goals that focus on oral motor skills and on drilling speech production. After the child meets a particular criterion level of speech accuracy mastery, grammatical goals are targeted in grammatical treatment. Such grammatical treatment often utilises grammatical recasts. Grammatical recasts have been found to be effective in facilitating grammar in a number of populations (Camarata, Nelson & Camarata, 1994; Nelson, Carskaddon & Bonvillian, 1973; Scherer & Olswang, 1989; Yoder, Spruytenburg, Edwards & Davies, 1995). A less commonly used type of recast, speech recast, has been shown to address speech accuracy and speech-comprehensibility goals. Using specific speech sounds as targets and speech recasts as the treatment, both infrequently and never-used speech sounds were acquired in intervention sessions and generalised to spontaneous speech samples with the mother or the clinician who did not treat the child (Camarata, 1993). These results were maintained 9 months after treatment and showed replication across subjects and behaviours. Similarly, children with co-occurring speech and language disorders have demonstrated faster responses to speech recasts than to imitation training (Smith & Camarata, 1999). Children with simultaneous deficits in speech, language, and cognitive domains have demonstrated increased speech accuracy and improved overall intelligibility when provided with sound-specific speech recasts (Koegel, Camarata, Koegel, Smith & Ben-Tal, 1998; Smith & Camarata, 1999) and with recasts targeting overall speech-comprehensibility (Camarata, Champion, Koegel, Koegel, Smith & Ben-Tal, 1997). In this latter study, the possible confound of increased familiarity with increased number of intervention sessions was controlled by transcribing the sessions in a random order.
It is important to note that the studies cited above have used either grammatical or speech recasts but not both in the same treatment session. If we could treat both grammatical and speech-comprehensibility goals within the same conversational treatment, both gains in both language domains may be more likely to become integrated into the child's language system and more likely to generalise to conversation. Additionally, the speech or language targets in the aforementioned studies were usually very specifically defined. For example, only child utterances that afford a very limited set of individual phonemes (e.g., 3 phonemic goals) to be modelled using speech recasts.
In order to improve the speech and language skills of children with Down syndrome in generalised, everyday contexts, it is important to use dependent measures that are likely to reflect socially valid changes in the child's skills. For example, dependent measures such as speech-comprehensibility and Mean Length of Utterance (MLU) should be examined with novel, untrained toys and with communication partners other than the clinician who worked directly with the child during intervention. Additionally, the interaction style in the generalisation sampling should not include recasts or the types of prompts that were used during treatment. Because the recast treatment employed herein parallels natural language acquisition, generalisation is often observed in studies of recast intervention (see Camarata & Nelson, in press).
Broad Target Recast (BTR) differs from other recasting treatments in that (a) both speech and grammatical recasts are used within the same treatment session and (b) almost all child utterances that afford developmentally appropriate grammatical or speech structures to be modelled in the recast are delivered. There has been one investigation into the effects of BTR. In a study of BTR in children with SLI, Yoder, Camarata and Gardner (2005) reported that BTR improved both speech-comprehensibility and MLU in a sample of children with co-morbid speech and language impairments who had particularly impaired speech accuracy prior to treatment onset. It is noteworthy that these effects were detected 8 months after the end of the treatment phase in rigorous generalisation sessions that were conversational language samples. Additionally, the transcriber was unfamiliar with the children, transcribed the sessions in a random sequence, and was blind to whether the session came from the pre-treatment, post-treatment or follow-up measurement periods. Although that study did not include children with Down syndrome, given the promising results in Yoder et al., (2005) and the evidence in support of recast style interventions in children with developmental disabilities, we hypothesised that children with Down syndrome may also improve speech and grammar abilities with BTR intervention.
The purpose of this study was to examine the effects of BTR on the speech-comprehensibility and utterance length of children with Down syndrome. The outcomes that were selected are at a level of detail that is arguably socially important and the measurement context is arguably similar to a frequent language-use context (i.e., conversations). Finally, the measurement context is a rigorous test of generalisation (across person, activity, and interaction style).
Methods
A multiple baseline, multiple probe design was used to examine the speech-comprehensibility and grammatical skills as measured using MLU in a total of six children with Down syndrome who were enrolled in a six month, twice weekly integrated speech-comprehensibility and language intervention programme. Two sets of 3 legs were used in the multiple baseline design to afford replication within and across sets of participants. The project manager was instructed to begin the treatment when there was a stable or downward trend in at least one of the two dependent variables with the provision that a staggered number of baseline sessions be used across individuals within the set. The dependent variables were measured in generalisation conversational samples.
Participants
Participants were six children with Down syndrome. This diagnosis was based upon the results of physician report. Within the broad range of medical conditions evident in Down syndrome, the participants were in good health and had major medical complications (e.g., heart defects) treated prior to enrolment in the project. In addition, the participants all had negative history for cleft palate and passed an audiometric screening. In addition, because the focus of this project was on speech-comprehensibility and grammar, all had MLUs above 1.0 and exhibited at least 20 utterances that were at least partially comprehensible in a 20-minute conversational sample.
The age range of these children was four years three months to seven years four months and included three females and three males. The mean age was 5.7 years with a standard deviation of 1.3 years in the participant group. In addition to the general eligibility criteria described above, the following measures were applied to all participants.
Mental age
The revised Leiter International Performance Scale (Roid & Miller, 1998) was administered to all participants. This is a standardised measure of nonverbal cognitive abilities that yields standard scores with a mean of 100 and a standard deviation of 15. The mean Leiter-R Score was 66.5 with a standard deviation of 5.0 for these participants.
Expressive and Receptive Language
The participants demonstrated a mean standard score on the grammatical morphology subtest of the Test of Auditory Comprehension of Language, Third Edition (TACL-3, Carrow-Woolfolk, 2001) of 63.0 with a standard deviation of 10.5. In addition, the MLU was a mean of 1.38 with a standard deviation of .41. The language sampling procedures are described below under dependent measures.
Dependent measures
The sampling context
Speech-comprehensibility and grammatical measures were derived from spontaneous speech and language samples collected in three to five baseline samples, and in six treatment sessions. These were conducted by staff other than the clinician who was providing intervention to the participant. This staff person had been trained to gather language samples using standard procedures in order to minimise variation between language samples within and across participants. The interaction style for these samples did not involve the use of recasts but included the use of topic continuing questions to ensure that sufficient opportunities for interaction were available to the children. These 20-minute samples included a standard set of toys to control for this factor between and within participants.
Grammatical variable
From the baseline and intervention phase language samples, Mean Length of Utterance in morphemes was derived. This variable was derived from the complete and comprehensible utterances with the aid of the Systematic Analysis of Language Transcripts (SALT, Miller & Chapman, 1993). MLU is a commonly used index of grammar. It has been shown to be very highly associated with a detailed measure of syntax (i.e., IPSYN), but is much less expensive to compute (Scarborough, Rescorla, Tager-Flusberg, Fowler & Sudhalter, 1991). Rondal et al., (1988) found that MLU significantly predicted age and syntactic complexity up to MLU of 3.0. Although MLU does not reflect the details of which aspects of grammar are mastered, it is a gross reflection of overall morpho-syntactic complexity during the period of development we studied (i.e., 1.0 - 3.0 MLU). Although MLU can be validly obtained using 50 utterances (Miller, 1981) we sought to obtain conversational samples with a minimum of 100 utterances to enhance stability for this metric. The actual number of utterances used to derive MLU ranged from 122 to 211 (M = 157, SD = 30.8). Initial MLU level was a mean of 1.38 with a standard deviation of .41.
Speech-comprehensibility
Percentage of utterances that were comprehensible was derived from baseline and intervention phase language samples. The actual percentage of communication units understood in a continuous speech sample were computed in the spontaneous samples (e.g., percentage of utterance attempts glossed) and may be among the most face-valid way to quantify what we are defining as speech-comprehensibility (see Kwiatkowski & Shriberg, 1992). This is arguably an ecologically valid measure because the inability to understand their children is often why parents bring their children to speech therapy. It is measured in a frequent speaking context for children with Down syndrome. Because such contexts are relatively uncontrolled, changes and treatment effects on this variable are arguably a conservative estimate. Initial speech-comprehensibility level was a mean of 46.56 percent with a standard deviation of 12.83
Interobserver agreement
The following reliability checks were completed. Having two orthographers transcribe the same videotape at different times and independently calculate the scores for these variables assessed reliability for MLU and speech-comprehensibility. Reliability coefficients for each measure were calculated using the proportion of agreement. For MLU, a proportion was generated by dividing the smaller MLU by the larger MLU in each pair of samples. Similarly, the proportion of agreement for percentage speech-comprehensibility was calculated using smaller percentage comprehensible divided by larger percentage comprehensible for each pair of samples. The advantage to this approach of estimating agreement is that we can use the same metric in the agreement estimation process as is used in the graphs to test the research questions. For MLU, the mean proportion agreement was .88 with an SD of .11. For speech-comprehensibility, the mean proportion of agreement was .72 with an SD = .26.
Recast intervention procedures
We posited that a naturalistic intervention in which staff-implemented speech and grammatical recasts were applied to children's non-imitative utterances would facilitate the children's grammatical and speech development. Verbal routines and questions were used to increase the probability of a comprehensible child platform utterance. A speech recast is an adult utterance that immediately follows a child utterance, gives a positive evaluation of the semantic content of the child's utterance, and is an exact or reduced imitation of the word(s) that the child attempted to say only using adult pronunciation of the attempted word. For example, if the child says, "This a wion [lion]," the recast might be "Yes, lion". Speech recasts are best used after interpretable, but poorly articulated child utterances in which substitutions or omissions occur (see Camarata & Nelson, in press). No new grammatical or semantic information is added to the child's utterance. Therefore, speech recasts will be grammatically similar to the child's form.
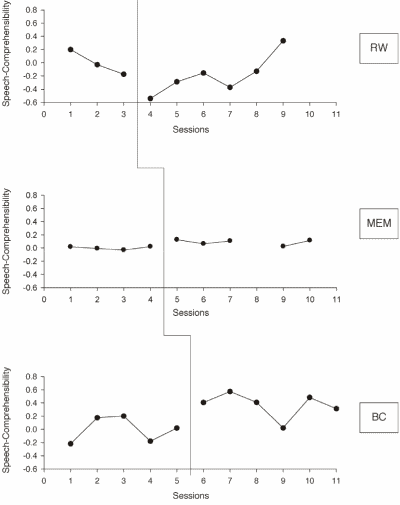
Figure 1 | Speech-Comprehensibility results for RW, MEM and BC
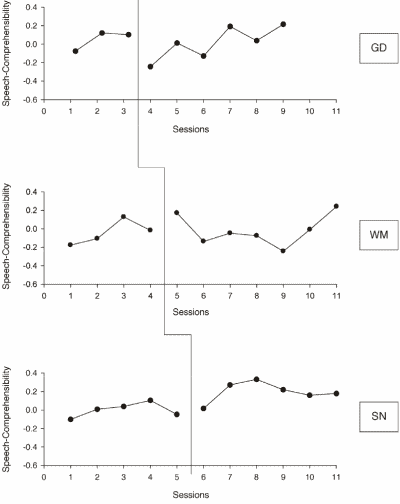
Figure 2 | Speech-Comprehensibility results for GD, WM and SN
Clinicians were trained to use both types of recasts to address the speech or grammatical structures that are missing or used in error in the child's platform utterance, as long as such are developmentally appropriate. We call such goals "broadly defined" intervention goals. We strive to deliver approximately 4 recasts per minute. The relative emphasis of speech and grammatical recasts varies according to the speech-comprehensibility of the child. Because speech-comprehensibility recasts are given to the least comprehensible utterances, frequently there is proportionally more speech recasting at the beginning of treatment than at the end.
Results
The plots for MLU and the speech-comprehensibility variables are provided in the figures. Because there were relatively large discrepancies in the baseline levels of MLU and percentage speech-comprehensibility within participants, the data were transformed as suggested by Kazdin (1984): (B i - Mb)/Mb wherein B i is the observed score and Mb is the mean baseline score for that participant on that dependent variable. This transformation thus provides a proportionally similar scale for data that are derived from participants with relatively large discrepancies in baseline scores. Such broad discrepancies can result in widely scattered scaling that can obscure important treatment effects (see Kazdin, 1984).
For the purposes of this study, growth is defined as an increase in mean levels of a dependent measure (i.e., MLU or speech-comprehensibility) during treatment when compared with that in the baseline phase. The results of the multiple baseline across subjects design indicated speech-comprehensibility growth in four (BC, GD, MEM and SN) of the six participants. Although the treatment mean was slightly higher than the baseline for RW as well, this was a very small difference and so not reported as evidence of growth. With respect to MLU, five (WM, BC, RW, MEM and SN) of the six participants showed growth. Thus, even using a relatively uncontrolled measurement context and broad indices of grammar and speech-comprehensibility (i.e., conservative measures of growth), there was evidence of growth in a majority of the participants on both dependent variables.
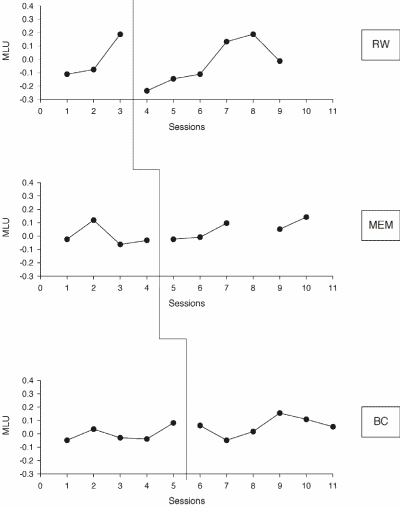
Figure 3 | MLU results for RW, MEM and BC
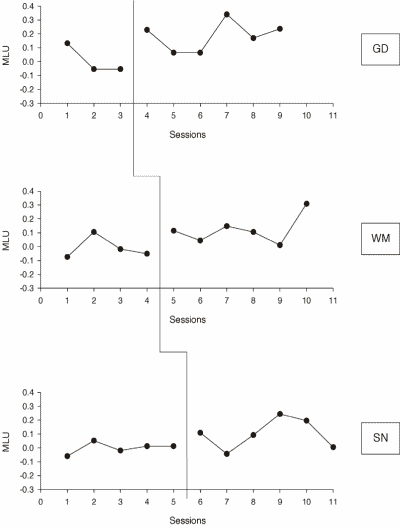
Figure 4 | MLU results for GD, WM and SN
However, determining intervention effects requires more stringent evidence than simply demonstrating growth. This requires stable baselines and a clear shift in the level, variability or slope of the dependent measure soon (within three sessions) after the onset of the treatment phase and clear separation of data points (in terms of overlap) in the baseline and intervention samples. Because our treatment phase contained six sessions, clear separation is defined here as no more than two (i.e., 33%) data points in the intervention phase overlapping with points in the baseline phase. Two of the participants showed evidence of treatment effects on speech-comprehensibility in generalisation sessions (BC and MEM). Similarly two (GD and SN) showed evidence of treatment effects on MLU in generalisation sessions.
Discussion
The results of this preliminary study suggest that recast intervention is promising for improving speech-comprehensibility and sentence length in children with Down syndrome. A cautious interpretation indicates that there was growth in speech-comprehensibility in 4/6 children and in MLU for 5/6 children. But, we wish to be careful in our interpretation of this finding: Growth is consistent with, but not necessarily evidence of, treatment effects as both of these variables are subject to maturational influences. Because we used a multiple baseline across subjects design, an intervention effect is defined as an immediate upward shift in the level, trend, or variability in dependent variable after the onset of the treatment and minimal overlap between baseline and intervention phases, assuming a stable baseline (Horner, Carr, Halle, McGee, Odom & Wolery, 2005). Under these conditions, one can be reasonably confident that some of the growth was caused by the intervention in a subset of children who showed growth. These criteria for identifying an intervention effect were met in two of these cases for speech-comprehensibility and MLU, respectively. We view this as a promising result for a number of reasons.
First, frequently experienced and arguably ecologically valid measurement contexts were used to measure the dependent variables: conversational samples. Second, socially important dependent variables were selected: Mean Length of Utterance (MLU) and percentage of utterance attempts that were comprehensible. But, because these are broad, ecologically valid measures and because the children in the study have mental retardation, the variables are also difficult to change rapidly after the onset of treatment. This type of rapid change in the dependent variable is required for experts in interpreting single subject data to agree that treatment effects have occurred (Parsonson & Baer, 1992). To illustrate this, consider the results presented in the Camarata (1993) pilot of phoneme specific recast to improve speech accuracy. In this research, target phonemes were at relatively low levels of percent accuracy, but most displayed some evidence of correct production in baseline. Following application of recast treatment, there were relatively rapid shifts in the percent accuracy for the targeted phonemes. One could argue that this more specific speech accuracy dependent variable is likely to shift more rapidly that the broader speech-comprehensibility measure employed in this study. Also, the data in Camarata (1993) were not derived from children with mental retardation, as was the case herein, so the changes may have been more rapid for this reason as well.
Second, speech-comprehensibility and MLU are well known to be particular challenges in people with Down syndrome (Miller & Leddy, 1999). The rationale for applying speech-comprehensibility rather than speech accuracy (as in Camarata, 1993) in Down syndrome bears some speculative discussion. It is striking that growth was observed in four of the six participants and two of these displayed treatment effects. It is important to bear in mind that no traditional articulation treatment (Bernthal & Bankson, 1999) was applied during this study. As Camarata (1995) notes, a focus on lexically based (word level) teaching models via recast de-emphasises phoneme specific speech accuracy training in favour of improved overall speech-comprehensibility. One could argue that children with Down syndrome are less likely than other children to benefit from phoneme level speech accuracy or oral-motor training because oral architecture and articulatory gestures may be quite different than other children. Additionally, such decontextualised training may result in little generalisation in children with mental retardation. Also, there is a clear need to study speech-comprehensibility, intelligibility and speech accuracy in Down syndrome and to specifically determine whether speech accuracy training ultimately yields improvements in intelligibility and speech-comprehensibility. Because of this, the results herein appear promising, as there was evidence of treatment effects in some of the participants for MLU and for speech-comprehensibility.
Finally, the study was designed as a preliminary investigation of a newly designed intervention to address a long-standing challenge in Down syndrome. The methods tested herein are relatively innovative, and frankly, an important part of this study was simply to test the feasibility of completing this kind of intervention in children with relatively low language levels and with low speech-comprehensibility. The results clearly demonstrate that the methods are feasible and the measures reasonable reliable.
This study should also be viewed in the context of directions for future research. A clear direction is to compare this method to articulation training for effects on speech-comprehensibility in children with Down syndrome within the context of a randomised clinical trial (RCT). This latter design is more likely than single subject techniques for determining treatment effects in variables such as MLU and speech-comprehensibility, which are likely to change slowly, especially in children with Down syndrome. RCTs do not require that the dependent variable change rapidly after the onset of treatment to detect a treatment effect. Also, such studies can and should include systematic measures of treatment fidelity for the contrasting conditions to ensure sharp procedural contrasts in the treatment conditions.
Similarly, it was clear that recast intervention was associated with changes in the outcomes in some children, but not others. We hypothesise that this will continue to be the case in future studies. That is, it is unlikely that one treatment will be effective with all children with Down syndrome. Therefore, treatment studies designed to detect individual differences in treatment response, and the pretreatment factors that predict such individual differences would be very useful (see Yoder & Compton, 2004).
Acknowledgements
The authors express appreciation to Mark Wolery, Robin Chapman and Lawrence Shriberg for helpful discussions during the development of this manuscript. Institutional support from the National Institutes of Health (Grant NICHD P3015052) to the Kennedy Center and the Scottish Rite Foundation of Nashville for this research is gratefully acknowledged. The work of the clinicians contributing to the research, including Frances Burns and Katherine Bush, is appreciated as is the technical support provided by Jon Tapp and Kylie Beck. We are also deeply appreciative of the parents and children who participated in the study. This research was funded by NICHD R03 HD042509. We would like to acknowledge Dr. Michael G. Davis. He was a co-investigator on the grant application.
Correspondence
Stephen Camarata • Director, Program in Communication & Learning, John F. Kennedy Center for Research on Development and Disabilities, Vanderbilt University, Nashville, Tennessee, USA 37232 • Stephen.m.camarata@vanderbilt.edu.
References
Bernthal, J. & Bankson, N. (1999). Articulation Disorders. Englewood Cliffs, NJ: Prentice-Hall.
Camarata, S. (1993). The application of naturalistic conversation training to speech production in children with speech disabilities. Journal of Applied Behaviour Analysis, 26, 173-182.
Camarata, S. (1995). A rationale for naturalistic speech intelligibility intervention. In M. Fey, J. Windsor & S. Warren (Eds.), Language Intervention: Preschool Through the Early School Years (pp. 63-84). Baltimore: Brookes.
Camarata, S. (1996). On the importance of integrating naturalistic language, social intervention, and speech-intelligibility training. In L. Koegel, R. Koegel & G. Dunlap (Eds.), Positive Behaviour Support (pp. 333-351). Baltimore: Brookes.
Camarata, S., Champion, T., Koegel, R., Koegel, L., Smith, A. & Ben-Tal, A. (1997). Speech Intelligibility Intervention in Children with Severe Speech Disorders. Paper presented at the annual convention of the American Speech-Language-Hearing Association.
Camarata, S., Nelson, K. & Camarata, M. (1994). A comparison of conversation based to imitation based procedures for training grammatical structures in specifically language impaired children. Journal of Speech and Hearing Research, 37, 1414 - 1423.
Camarata, S., Nelson, K. & Camarata, M. (1996). On the importance of providing detailed procedural descriptions in treatment research. Journal of Speech and Hearing Research, 39, 222-223.
Camarata, S. and Nelson, K. (in press). Preschool language intervention. In R. McCauley & M. Fey (Eds.), Language Intervention. Brookes Publishing.
Carrow-Woolfolk, E. (2001). Test of Auditory Comprehension of Language, third edition. Circle Pines, MN: American Guidance Service (AGS).
Chapman, R. (1995). Language development in children and adolescents with Down syndrome. In P. Fletcher and B. MacWhinney (Eds.), Handbook of Child Language (pp. 641- 663). Oxford, England: Blackwell Publishers.
Chapman, R., Kay-Raining Bird, E. & Schwartz, S. (1990). Fast mapping of words in event contexts by children with Down syndrome. Journal of Speech and Hearing Disorders, 55, 761-770.
Chapman, R., Kay-Raining Bird, E. & Schwartz, S. (1991, November). Fast Mapping in Stories: Deficits in Down Syndrome. Paper presented at the annual convention of the American Speech Language Hearing Association, Atlanta, GA.
Chapman, R., Seung, H., Schwartz, S. & Kay-Raining Bird, E. (2000). Predicting language production in children and adolescents with Down syndrome: The role of comprehension. Journal of Speech, Language, and Hearing Research, 43(2), 340-350.
Chapman, R., Streim, N., Crais, E., Slamon, D., Negri, N. & Strand, E. (1992). Child talk: Assumptions of a developmental process model for early language learning. In R.S. Chapman (Ed.), Processes in Language Acquisition and Disorders (pp. 3-9). Chicago: Mosby-Yearbook.
Foster, J. & Afzalnia, M. (2005). International assessment of judged symbol comprehensibility. International Journal of Psychology, 40, 169-175
Gordon-Brannan, M. & Hodson, B. (2000). Intelligibility-Severity measurements of prekindergarten children's speech. American Journal of Speech-Language Pathology, 9, 141-150.
Hanson, E., Yorkston, K. & Beukelman, D. (2004). Speech Supplementation Techniques for Dysarthria: A Systematic Review. Journal of Medical Speech Language Pathology, 12, 9-26.
Horner, R., Carr, E., Halle, J., McGee, G., Odom, S. & Wolery, M. (2005). The use of single subject research to identify evidence-based practice in special education. Exceptional Children, 71, 165-179.
Kazdin, A. (1984). Statistical analyses for single-cases experimental designs. In D. Barlow & M. Hersen (Eds.), Single Case Experimental Designs (pp. 285-324). Boston, MA: Allyn & Bacon.
Koegel, R., Camarata, S., Koegel, L., Smith, A. & Ben-Tal, A. (1998). Improving speech in children with autism. Journal of Autism and Developmental Disabilities, 28, 241-251.
Kent, R.D., Miolo, G. & Bloedel, S. (1994). The intelligibility of children's speech: A review of evaluation procedures. American Journal of Speech-Language Pathology, 3, 31-95.
Kent, R.D., Weismer, G., Kent, J. & Rosenbek, J. (1989). Toward phonetic intelligibility testing in dysarthria. Journal of Speech & Hearing Disorders, 54, 482-499.
Leddy, M. (1999). Biological bases of speech in people with Down syndrome. J. Miller, M. Leddy & L. Leavitt (Eds.), Improving the Communication of People with Down Syndrome (pp. 61-80).
Leonard, L., Camarata, S., Brown, B. & Camarata, M. (in press). Tense and agreement in the speech of children with specific language impairment: Patterns of generalisation through intervention. Journal of Speech-Language-Hearing Research.
Leonard, L., McGregor, K. & Allen, G. (1992). Grammatical morphology and speech perception in children with specific language impairment. Journal of Speech and Hearing Research, 35, 1076-1085.
Miller, J. (1999). Profiles of language development in children with Down syndrome. In J. Miller, M. Leddy & L. Leavitt (Eds.), Improving the Communication of People with Down Syndrome (pp. 11-40).
Miller, J. & Chapman, R. (1993). SALT: Systematic Analysis of Language Transcripts. Madison, WI: University of Wisconsin.
Miller, J. & Leddy, M. (1999). Verbal fluency, speech intelligibility, and communicative effectiveness. In J. Miller, M. Leddy & L. Leavitt (Eds.), Improving the Communication of People with Down Syndrome (pp. 81-91).
Nelson, K.E. (1989). Strategies for first language teaching. In M. Rice & R. Schiefelbush (Eds.), Teachability of Language (pp. 263-310). Baltimore: MD: Paul Brookes.
Nelson, K., Carskaddon, G. & Bonvillian, J. (1973). Syntax acquisition: Impact of experimental variation in adult verbal interaction with the child. Child Development, 44, 497-504.
Nelson, K.E. (1977). Facilitating children's syntax acquisition. Developmental Psychology, 13, 101-107.
Parsonson, B. & Baer, D. (1992). The visual analysis of data, and current research into the stimuli controlling it. In T. Kratochwill and J. Levin (Eds.), Single-case Research Design and Analysis (pp. 15-40). Hillsdale: Erlbaum.
Proctor-Williams, K., Fey, M. & Frome-Loeb, D. (2001). Parental recasts and production in copulas and articles by children with specific language impairment and typical language. American Journal of Speech Language Pathology, 10, 155-168.
Roid, G. & Miller, L. (1997). Leiter International Performance Scale - Revised. Wood Dale, IL: Stoelting, Co.
Rondal, J., Ghiotto, M., Bredart, S. & Bachelet, J.(1988). Mean length of utterance of children with Down syndrome. American Journal on Mental Retardation, 93, 64-66.
Scarborough, H., Rescorla, L., Tager-Flusberg, H., Fowler, A. & Sudhalter, V. (1991). The relation of utterance length to grammatical complexity in normal and language-disordered groups. Applied Psycholinguistics, 12, 23-45.
Scherer, N. & Olswang, L. (1989). Using structured discourse as a language intervention technique with autistic children. Journal of Speech and Hearing Disorders, 54, 383-394.
Shatz, M. (1983). Communication. In P.H. Mussen (Ed.), Handbook of Child Psychology. Vol III: Cognitive Development ( pp. 841-889). New York: Wiley & Sons.
Shriberg, L.D. & Kwiatkowski, J. (1982). Phonological disorders III: A procedure for assessing severity of involvement. Journal of Speech & Hearing Disorders, 47, 256-270.
Shriberg, L.D., Kwiatkowski, J., Best, S., Hengst, J. & Terselic-Weber, B. (1986). Characteristics of children with phonologic disorders of unknown origin. Journal of Speech and Hearing Disorders, 51(2), 140-161.
Smith, A. & Camarata, S. (1999). Increasing language intelligibility of children with autism within regular classroom settings using teacher implemented instruction. Journal of Positive Behaviour Intervention, 1, 141-151.
Yoder, P., Camarata, S. & Gardner, E. (2005). Treatment effects on speech intelligibility and length of Utterance in children with specific language and intelligibility impairments. Journal of Early Intervention, 28 , 34-49.
Yoder, P. & Compton, D. (2004). Identifying Predictors of Treatment Response. Mental Retardation and Developmental Disabilities Research Reviews, 10, 162-168.
Yoder, P.J. & Davies, B. (1992a). Do children with developmental delays use more frequent and diverse language in verbal routines? American Journal of Mental Retardation, 97(2) , 197-208.
Yoder, P.J. & Davies, B. (1992b). Greater intelligibility in verbal routines with young children with developmental delays. Applied Psycholinguistics, 13, 77-91.
Yoder, P.J., Spruytenburg, H., Edwards, A. & Davies, B. (1995). Effect of verbal routine contexts and expansions on gains in the mean length of utterance in children with developmental delays. Language, Speech, Hearing Services in Schools, 26, 21-32.

